
Quick Summary: Transgender men and nonbinary people who were assigned female at birth and retain a uterus and ovaries can become pregnant. Cisgender men—those born with male reproductive anatomy—cannot currently become pregnant, though emerging uterine transplant research may change this in the future. Research published in medical journals shows that pregnancy is possible for transgender men, even for some who have used testosterone therapy.
The question “can men get pregnant” depends entirely on what reproductive anatomy someone has—not their gender identity. This distinction matters because pregnancy is increasingly common among transgender men and nonbinary individuals.
Gender identity doesn’t determine reproductive capacity. Biology does.
But here’s where it gets interesting. Medical research shows pregnancy outcomes for transgender men mirror those of cisgender women in many ways, while emerging technologies like uterine transplants could eventually make pregnancy possible for cisgender men too.
Who Can Actually Become Pregnant
Pregnancy requires specific reproductive organs: a uterus and ovaries. Any person who has these organs can potentially become pregnant, regardless of their gender identity or how they present to the world.
Transgender men—people assigned female at birth who identify as men—can become pregnant if they still have their uterus and ovaries. The same applies to many nonbinary individuals.
According to the World Health Organization, reproductive health encompasses the capability to reproduce and the freedom to decide if, when, and how often to do so. This definition deliberately uses gender-neutral language because reproductive capacity isn’t confined to women.
The Role of Reproductive Anatomy
Research published by the National Institutes of Health confirms that pregnancy depends on having functional reproductive organs, not gender identity. The uterus provides the environment where a fertilized egg implants and develops. The ovaries produce eggs and hormones necessary for conception and early pregnancy.
Some transgender men undergo surgery to remove these organs as part of gender-affirming care. But many don’t—either by choice or because they haven’t yet accessed surgical options.
And that means pregnancy remains biologically possible.
Transgender Men and Pregnancy: What Research Shows
Medical literature documents numerous cases of transgender men achieving pregnancy. A 2014 study surveyed 41 transgender men and gender nonconforming individuals who became pregnant and gave birth.
The findings challenged common misconceptions.
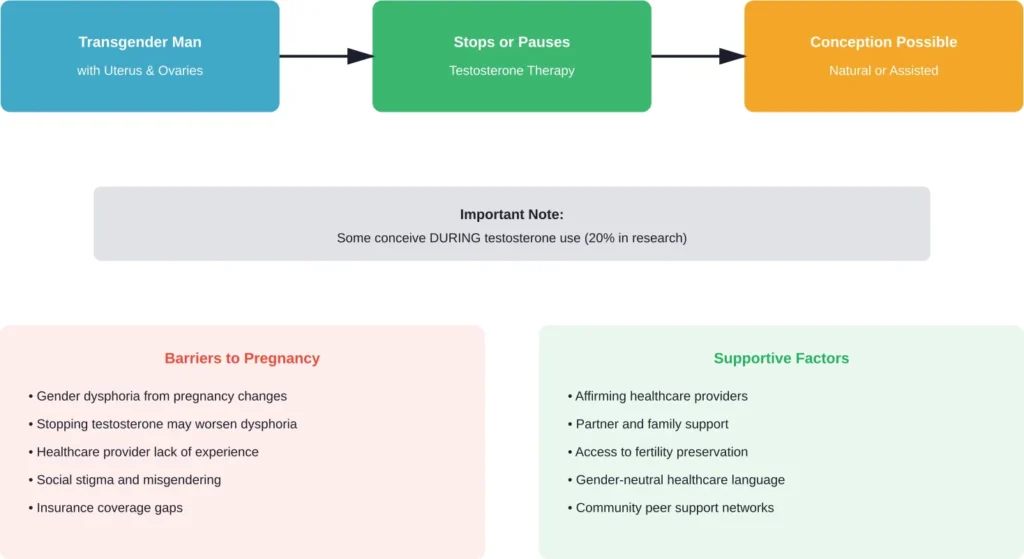
Of the participants who had used testosterone therapy before pregnancy, 20% conceived before their menstrual cycle returned. This suggests testosterone doesn’t provide reliable contraception—a critical fact that’s not widely known.
Research published in NIH databases shows pregnancy is achievable for transgender men who have received gender-affirming hormone therapy, even without fertility-preserving measures beforehand. Some individuals conceive naturally after stopping testosterone, while others require reproductive assistance.
How Testosterone Affects Fertility
Testosterone therapy typically causes amenorrhea—the absence of menstrual periods. Many people mistakenly believe this means they can’t get pregnant.
Wrong.
A 25-year-old transgender man receiving testosterone treatment became pregnant despite ongoing hormone therapy, according to case reports in medical journals. The therapy had caused amenorrhea, leading him to believe contraception wasn’t necessary.
Testosterone may reduce fertility, but it doesn’t eliminate it. After stopping testosterone, many transgender men regain fertility as their menstrual cycles resume—though the timeline varies significantly between individuals.
Fertility Treatment Outcomes for Trans Men
Research examining in vitro fertilization (IVF) outcomes for transgender men shows encouraging results. Studies found no correlation between time on or off testosterone therapy and the number of eggs retrieved during IVF cycles.
All patients who completed IVF or embryo cryopreservation produced high-quality blastocysts. This suggests testosterone exposure doesn’t permanently damage reproductive capacity in most cases.
Ovarian response to fertility medications appears normal in transgender men who previously used testosterone, according to data from reproductive medicine clinics. Treatment outcomes mirror those of cisgender women in similar age groups.
The Experience of Pregnancy for Transgender Men
Pregnancy presents unique challenges for transgender men beyond the biological aspects. The social association of pregnancy with femininity can trigger or worsen gender dysphoria—the distress caused by a mismatch between gender identity and assigned sex at birth.
But not everyone experiences it this way.
Some transgender men report feeling comfortable with pregnancy, viewing it as a separate process from their gender identity. Others find it deeply distressing. There’s no universal experience.
Research with transgender men who experienced pregnancy identified several recurring themes. Ceasing testosterone often exacerbates dysphoria. Healthcare appointments can involve repeated misgendering. Finding supportive providers remains difficult in many areas.
Mental Health Considerations
The intersection of pregnancy and gender identity requires careful mental health support. Some transgender men feel isolated because pregnancy resources overwhelmingly use feminine language and imagery.
Think about it. Prenatal classes talk about “mothers-to-be.” Products feature exclusively feminine marketing. Medical forms often lack options beyond “mother” and “father.”
This erasure matters. Studies document how inclusive language improves healthcare experiences for transgender patients. Simple changes—like “pregnant people” instead of “pregnant women”—make clinical spaces more welcoming.
| Exclusive Language | Inclusive Alternative |
|---|---|
| Pregnant women | Pregnant people |
| Mothers-to-be | Expectant parents |
| Breastfeeding mothers | Chestfeeding parents |
| Women seeking abortion | People seeking abortion |
| Maternal health | Perinatal health |
Can Cisgender Men Get Pregnant?
Currently, no. Cisgender men—people assigned male at birth who identify as men—lack the uterus and ovaries necessary for pregnancy.
That biological reality holds true regardless of advances in other areas of medicine.
But emerging research on uterine transplants suggests this might change. Scientists are exploring whether transplanting a uterus into someone born with male anatomy could enable pregnancy.
Uterine Transplant Research
Uterine transplants have enabled successful pregnancies and births in cisgender women, with multiple cases documented worldwide. Since then, dozens of babies have been born worldwide through this procedure. The uterus is transplanted, pregnancy is achieved through IVF, and the uterus is typically removed after delivery to avoid lifelong immunosuppression.
Could this work for cisgender men or transgender women? Theoretically, yes. Practically, researchers face significant hurdles.
The male pelvis has a different shape. Hormone regimens would need adjustment. Vascular connections pose technical challenges. And ethical questions abound about the risks involved.
Still, some researchers believe male pregnancy through uterine transplant could become reality within the next decade or two. The science isn’t there yet—but it’s not science fiction either.
Male Infertility and Reproductive Health
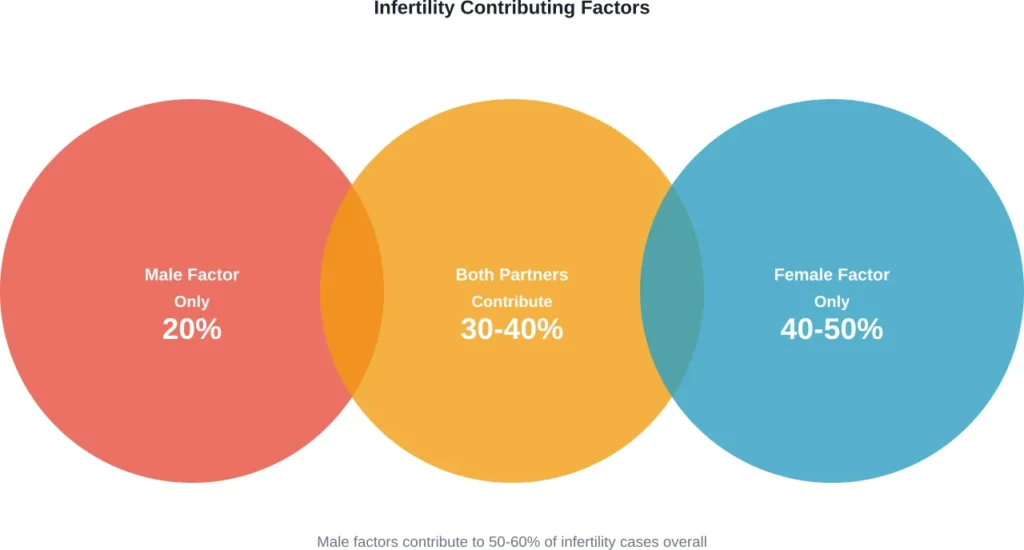
While discussing who can get pregnant, it’s worth addressing male infertility—a factor in 40-50% of couples struggling to conceive.
According to the World Health Organization, infertility affects approximately one in six people of reproductive age worldwide. Male infertility specifically involves problems with sperm production, function, or delivery.
Common Causes of Male Infertility
The NIH identifies several primary causes. Varicoceles—enlarged veins in the scrotum—affect sperm production. Infections can interfere with sperm health. Ejaculation problems prevent sperm delivery. Hormonal imbalances reduce sperm production.
Research shows male infertility is solely responsible for about 20% of cases where couples can’t conceive. In another 30-40% of cases, both partners contribute factors that affect fertility.
This matters because discussions of pregnancy often focus exclusively on people with uteruses. But conception requires contribution from both partners, and male factors significantly impact reproductive outcomes.
Singapore’s Fertility Research Insights
Recent research initiatives highlight the importance of studying male reproductive health. Singapore’s TOFFFY study (Towards Optimal Fertility, Fathering, and Fatherhood) was published in January 2025 to investigate male factors and their relationships with reproductive health outcomes.
This comes as Singapore faces a total fertility rate below 1.0—among the lowest globally. The research recognizes that despite comprehensive pronatalist policies, male contributions to fertility remain understudied.
The study protocol, published in BMJ Open in January 2025, emphasizes that low fertility rates can’t be addressed by focusing solely on people with uteruses. Conception requires healthy contributions from all partners involved.
Healthcare Access and Inclusive Practices
Access to gender-affirming reproductive healthcare varies dramatically by location. Many transgender men report difficulty finding providers knowledgeable about their specific needs during pregnancy.
Standard prenatal care often assumes all pregnant patients are cisgender women. Forms, language, and even physical spaces may not accommodate transgender men or nonbinary individuals.
Real talk: healthcare systems need to catch up with the reality that diverse people experience pregnancy.
What Inclusive Healthcare Looks Like
Reproductive healthcare providers increasingly recognize the need for inclusive practices. This includes using gender-neutral intake forms, offering private changing areas, and training staff on appropriate language.
Medical facilities serving transgender patients should ask for pronouns and chosen names. Electronic health records should accommodate gender identity separate from sex assigned at birth. Providers should be prepared to address unique concerns like chest dysphoria during nursing.
Some clinics now use terms like “chestfeeding” instead of “breastfeeding” to better describe the experience of transgender men who feed their infants. This small change acknowledges that not everyone who lactates identifies as a woman or has breasts they’re comfortable naming.
Abortion Access for Transgender Men
Discussions about pregnancy must include abortion access. Transgender men face unique barriers when seeking reproductive healthcare, including abortion services.
Clinic staff may lack training on serving transgender patients. Waiting rooms designed exclusively for women can feel unwelcoming or unsafe. Legal documentation requirements may force patients to out themselves.
Some jurisdictions with abortion restrictions specifically mention “women,” creating legal ambiguity about whether the laws apply to transgender men. This uncertainty can delay or prevent access to time-sensitive care.
Personal Stories and Lived Experiences
Research with transgender men who’ve experienced pregnancy reveals diverse perspectives. Some describe pregnancy as empowering—a way to build their family that aligns with their values despite social expectations.
Others find it traumatic, citing dysphoria, medical mistreatment, or social isolation.
One consistent theme emerges: the importance of choice. Transgender men who feel supported in their decision—whether to pursue pregnancy, avoid it, or terminate it—report better mental health outcomes than those who feel pressured or judged.
Community discussions highlight the need for peer support. Connecting with other transgender people who’ve navigated pregnancy can provide validation and practical advice that cisgender providers may not offer.
Future Possibilities in Reproductive Medicine
Medical advances continue expanding reproductive options. Beyond uterine transplants, researchers explore ectogenesis—developing fetuses outside the human body in artificial wombs.
While still largely theoretical for human use, this technology could eventually enable biological parenthood for people without any reproductive organs. It might also reduce pregnancy-related health risks for all people.
Advances in fertility preservation improve options for transgender individuals considering medical transition. Egg freezing before starting testosterone allows transgender men to preserve fertility while pursuing gender-affirming care.
Ethical Considerations
These possibilities raise complex ethical questions. Who should have access to emerging reproductive technologies? How do we balance innovation with safety? What are the long-term effects of growing in artificial environments?
Questions without easy answers. But they’re worth grappling with as technology outpaces policy and cultural understanding.
Practical Guidance for Trans People Considering Pregnancy
For transgender men and nonbinary people considering pregnancy, preparation matters. Finding affirming healthcare providers before conception improves outcomes.
Questions to ask potential providers: Do they have experience with transgender patients? What pronouns and names will appear on medical records? How do they handle insurance billing for gender-affirming care?
Consider the mental health impact. Pregnancy may trigger dysphoria, and stopping testosterone can worsen it. Having a therapist familiar with gender identity issues provides crucial support.
Fertility Preservation Options
For those starting testosterone who want biological children later, egg freezing offers insurance. The process involves hormonal stimulation to produce multiple eggs, which are then harvested and frozen.
Cost varies significantly by location and clinic, with expenses for egg freezing and storage. Insurance coverage remains inconsistent—some plans cover fertility preservation before transition, others don’t.
| Consideration | Before Testosterone | After Testosterone |
|---|---|---|
| Fertility Status | Typically normal | Reduced but often recoverable |
| Preservation Options | Egg freezing, embryo freezing | Same, after recovery period |
| Conception Timeline | Immediate possibility | May require stopping testosterone |
| Medical Monitoring | Standard fertility care | Requires trans-competent providers |
The Role of Language in Reproductive Health
Language shapes healthcare experiences. When medical materials exclusively reference “women” and “mothers,” transgender men become invisible.
This isn’t about political correctness. It’s about health outcomes.
Studies show that inclusive language correlates with better patient satisfaction, treatment adherence, and health outcomes. When patients feel seen and respected, they’re more likely to seek preventive care and follow medical advice.
Healthcare institutions increasingly adopt inclusive terminology. The WHO’s definitions of reproductive health deliberately avoid gender-specific language, recognizing that reproductive capacity exists across gender identities.
Frequently Asked Questions
No, cisgender men lack the uterus and ovaries necessary for pregnancy. However, emerging uterine transplant research may eventually make pregnancy possible for people born with male anatomy, though this remains experimental and years away from clinical reality.
Not always. While stopping testosterone increases fertility and is generally recommended, research shows that 20% of transgender men in one study conceived before their menstrual cycles returned. Testosterone isn’t reliable contraception, and pregnancy can occur during therapy.
Generally speaking, testosterone doesn’t cause permanent infertility. Many transgender men regain fertility after stopping testosterone, though the timeline varies. Research on IVF outcomes shows transgender men who previously used testosterone produce eggs and embryos comparable in quality to those of cisgender women.
Pregnant transgender men face similar medical risks as cisgender women, including gestational diabetes and preeclampsia. Additional considerations include mental health challenges like gender dysphoria and potential barriers to accessing affirming healthcare. Finding providers experienced with transgender pregnancy improves outcomes.
Yes, many transgender men can chestfeed, though this depends on whether they’ve had chest surgery and personal comfort level. Those who haven’t had top surgery typically retain the ability to lactate. Some experience dysphoria with chestfeeding, while others find it affirming.
Medical research indicates pregnancy outcomes for transgender men are generally similar to those of cisgender women. Studies examining complications, delivery methods, and infant health show no significant differences attributable to transgender identity or prior testosterone use.
Start by contacting LGBTQ+ health centers, which often maintain referral lists of trans-competent providers. Online directories and community recommendations help identify affirming practitioners. When interviewing potential providers, ask directly about their experience with transgender pregnancies and their approach to inclusive care.
Conclusion: Expanding Our Understanding of Pregnancy
The question “can men get pregnant” has a nuanced answer that reflects evolving understanding of gender and reproductive biology. Transgender men and nonbinary people can and do become pregnant when they retain the necessary reproductive anatomy.
For cisgender men, pregnancy remains biologically impossible with current technology—though research into uterine transplants suggests this could change within coming decades.
What matters most? Recognizing that reproductive capacity doesn’t determine gender identity, and that healthcare systems must serve all people who experience pregnancy, regardless of how they identify.
The medical community increasingly acknowledges that inclusive language and affirming care improve outcomes. As research continues expanding knowledge about transgender reproductive health, the gap between policy, practice, and patient needs should narrow.
Whether someone identifies as male, female, nonbinary, or any other identity, their reproductive choices deserve respect and support. Healthcare providers, policymakers, and communities all play roles in creating environments where everyone can make informed decisions about their bodies and futures.
If you’re a transgender man or nonbinary person considering pregnancy, seek out affirming healthcare providers and community support. If you’re a healthcare worker, commit to inclusive practices that serve all patients with dignity. And if you’re simply learning about this topic, remember: expanding our understanding of who can become pregnant doesn’t diminish anyone’s experience—it simply acknowledges the full reality of human diversity.