Quick Summary: No, healthy males cannot truly run out of sperm. The body continuously produces sperm through spermatogenesis, a process taking roughly 64 days on average, with an additional 14 days for maturation in the epididymis (totaling approximately 74-78 days). While ejaculate volume or sperm count may temporarily decrease with frequent ejaculation, production never completely stops in healthy individuals.
It’s a question that crosses many minds, especially for those trying to conceive or simply curious about their reproductive health: can you actually run out of sperm?
The short answer is no. But there’s more to the story than that simple reassurance.
Understanding how the male body produces sperm, what’s actually in semen, and what might cause changes in ejaculate can clear up confusion and address legitimate health concerns.
How Sperm Production Actually Works
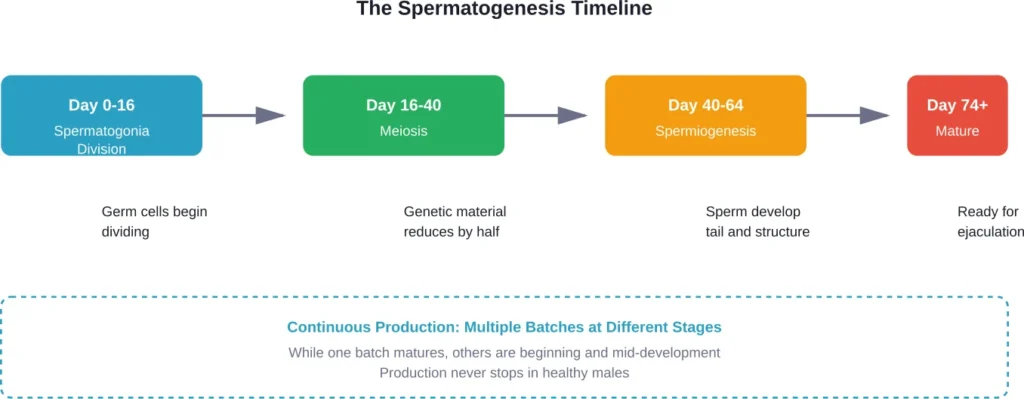
Sperm production happens through a process called spermatogenesis. According to the National Institutes of Health, this occurs in the seminiferous tubules inside the testes, where germ cells develop into mature sperm cells.
The entire production cycle takes roughly 64 days on average, with an additional 14 days for maturation in the epididymis (totaling approximately 74-78 days). That means from the moment a germ cell begins developing, it takes about two to two and a half months to become a fully mature sperm ready for ejaculation.
Here’s the thing though—this process isn’t happening in isolation. While one batch of sperm is maturing, another is just beginning development, and yet another is nearing completion. Production runs continuously, like a factory with multiple assembly lines operating simultaneously.
According to the NIH, apoptosis or degeneration results in the loss of about 75% of the germ cells that have developed. Only 25% of the germ cells reach the ejaculate, and research reveals that about 50% are malformed.
Sound inefficient? Perhaps. But the sheer volume of production compensates for this loss.
What’s Actually in an Ejaculate
When people worry about running out of sperm, they’re often confusing sperm cells with semen—the fluid that carries them.
Semen is a mixture, and sperm cells represent only a small fraction of the total volume. The seminal vesicles contribute approximately 65-75% of ejaculate volume, while the prostate adds another 25-30%. The remaining portion includes secretions from the bulbourethral glands and the sperm themselves.
| Component | Percentage of Volume | Primary Function |
|---|---|---|
| Seminal vesicle fluid | 65-75% | Provides fructose for energy, prostaglandins |
| Prostatic fluid | 25-30% | Contains enzymes, zinc, citric acid |
| Sperm cells | <5% | Fertilization |
| Bulbourethral glands | <1% | Pre-ejaculate, lubrication |
This composition explains why someone might notice changes in ejaculate volume without necessarily having a sperm production problem.
Does Frequent Ejaculation Deplete Sperm?
Ejaculating frequently can temporarily reduce sperm concentration per ejaculate. But this isn’t the same as running out.
Think of it like this: if production is constant but withdrawal increases, each individual sample contains fewer mature sperm simply because there’s been less time to accumulate. The factory is still running at full capacity—you’re just collecting from the output more often.
Research on spermatogenesis recovery has documented cases where sperm counts can rebuild relatively quickly. One case study published in Clinical Case Reports documented spermatogenesis recovery from zero to almost 16 million sperms per milliliter in less than four months after cessation of steroid cycles in a 44-year-old healthy man.
For most healthy individuals, waiting 2-3 days between ejaculations allows sperm concentration to normalize. Waiting longer doesn’t necessarily improve quality, though—sperm that sit too long in the epididymis can accumulate DNA damage.
When Ejaculate Contains No Sperm
Now, there are legitimate medical conditions where semen contains little or no sperm. This is called azoospermia, and it affects about 1% of all males and approximately 15% of infertile men.
Azoospermia has two main types:
Obstructive azoospermia means sperm are being produced, but a blockage prevents them from reaching the ejaculate. Causes include vasectomy, congenital absence of the vas deferens, or scarring from infection.
Non-obstructive azoospermia means production itself is impaired. This can result from hormonal issues, genetic conditions, varicoceles (enlarged veins in the scrotum with a prevalence around 20% according to the American Urological Association), or testicular damage.
According to the WHO, infertility affects approximately 1 in 6 people of reproductive age worldwide. Male factor substantially contributes to about 50% of all cases of infertility, with the male solely responsible in about 20% of cases and contributing to another 30-40%.
Dry Orgasm: When Nothing Comes Out
Sometimes the concern isn’t about sperm count but about ejaculate not appearing at all. This is called a dry orgasm.
A dry orgasm doesn’t mean sperm production has stopped. Several factors can cause this:
- Retrograde ejaculation: Semen travels backward into the bladder instead of out through the urethra
- Medication side effects: Certain medications, particularly some used for prostate conditions or mental health
- Surgery: Procedures affecting the prostate, bladder neck, or surrounding structures
- Neurological conditions: Diabetes, spinal cord injuries, or multiple sclerosis
The orgasm itself can still occur normally—it’s just the ejaculate that’s absent or redirected.
Factors That Actually Affect Sperm Health
While production continues throughout adult life, quality and quantity can vary based on several factors.
Age: While men don’t experience a sharp fertility decline like menopause, sperm quality does gradually decrease with age. Production continues, but DNA fragmentation and motility issues become more common.
Temperature: The testes hang outside the body for a reason—sperm production requires temperatures slightly below core body temperature. Frequent hot tub use, tight clothing, or laptop heat can temporarily impair production.
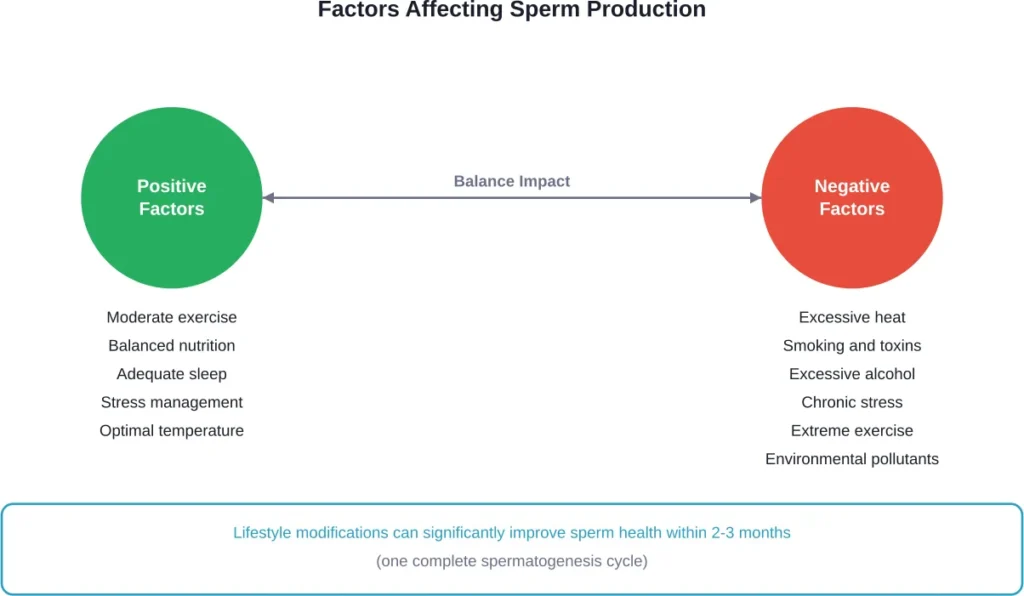
Lifestyle factors: According to competitor analysis, moderate exercise improves sperm health, while excessive training can damage it. Exposure to pollutants including heavy metals, tobacco smoke, pesticides, and endocrine disruptors also negatively impacts production.
Medical conditions: Varicoceles, hormonal imbalances, infections, and certain medications can all reduce sperm count or quality.
Nutrition: Deficiencies in key nutrients like zinc, folate, and antioxidants can impair spermatogenesis.
When to Seek Medical Evaluation
So when should someone actually worry about sperm production?
The WHO and American Urological Association recommend seeking evaluation if a couple has been trying to conceive for 12 months without success (or 6 months if the female partner is over 35).
Other warning signs include:
- Noticeable changes in testicular size or shape
- Pain or swelling in the testicular area
- Difficulty achieving or maintaining erections
- Changes in sexual desire
- Sudden onset of dry orgasms without explanation
- History of testicular injury, surgery, or cancer
A semen analysis provides the baseline data. The WHO laboratory manual specifies what’s measured: sperm concentration, total count, motility, morphology, and various other parameters. Normal values vary, but generally a concentration above 15 million sperm per milliliter is considered adequate.
The Bottom Line on Sperm Depletion
Real talk: barring serious medical conditions, healthy males maintain sperm production from puberty through old age.
Production might slow. Quality might decline. Individual ejaculates might contain fewer sperm after frequent sexual activity. But the fundamental process continues.
The body is remarkably resilient. Even after factors that temporarily suppress production—certain medications, illness, or environmental exposures—spermatogenesis typically resumes once the factor is removed, often within a few months.
That said, sperm health matters for fertility and potentially for offspring health. Taking steps to optimize production through lifestyle modifications, avoiding known toxins, and managing underlying health conditions makes physiological sense.
Frequently Asked Questions
Sperm production is continuous, taking 64-74 days for a complete cycle. However, sperm concentration in ejaculate typically normalizes within 2-3 days after ejaculation. The body maintains reserves in the epididymis, so immediate depletion doesn’t occur.
No. Frequent masturbation may temporarily reduce sperm concentration per ejaculate, but it doesn’t stop production. The testes continue generating new sperm continuously. Some evidence suggests that regular ejaculation (2-3 times per week) may actually support better sperm quality by preventing accumulation of aged sperm.
Dry orgasm (no ejaculate) can result from retrograde ejaculation (semen going into the bladder), certain medications, prostate or bladder surgery, or neurological conditions. This is different from low sperm count—the fluid itself is absent or redirected, not just the sperm cells.
Yes, gradually. Men don’t stop producing sperm, but volume, concentration, motility, and genetic quality typically decline with age. These changes accelerate after age 50, though many older men maintain adequate fertility. The decline is much more gradual than female age-related fertility changes.
Key steps include maintaining a healthy weight, exercising moderately, avoiding excessive heat to the testicles, eating a nutrient-rich diet with antioxidants, managing stress, getting adequate sleep, avoiding tobacco and excessive alcohol, and minimizing exposure to environmental toxins. Results typically appear after one complete production cycle (2-3 months).
Non-obstructive azoospermia can result from hormonal disorders, genetic conditions like Klinefelter syndrome, chemotherapy or radiation, severe varicoceles, testicular failure, or certain medications. Obstructive azoospermia (sperm produced but blocked) can occur from vasectomy, infections, congenital absence of vas deferens, or scarring.
Moderate abstinence (2-3 days) typically optimizes sperm count for conception attempts. Longer periods don’t necessarily help—sperm quality may decline with prolonged storage. Shorter intervals may reduce concentration but usually maintain adequate numbers for fertilization in healthy individuals.
Moving Forward
Understanding sperm production removes unnecessary anxiety while highlighting when professional evaluation makes sense.
The male reproductive system is built for continuous output. Temporary fluctuations are normal. But persistent changes, difficulty conceiving, or concerning symptoms warrant medical attention.
Semen analysis provides objective data. Lifestyle modifications offer improvement potential. And for most people wondering if they can run out—the answer remains a reassuring no.
If concerns about fertility or reproductive health persist, consult a urologist or reproductive endocrinologist. Evidence-based evaluation beats speculation every time.