
Quick Summary: While true water allergy doesn’t exist in the traditional sense, aquagenic urticaria is a rare condition where skin contact with water causes painful hives and itching. About 50 cases have been reported in the medical literature, and it’s not an immune response to water itself but rather a reaction to compounds that form when water contacts the skin. Treatment focuses on symptom management with antihistamines.
Imagine taking a shower and breaking out in painful, itchy hives. Or crying and feeling your own tears burn your face. For people with aquagenic urticaria, this nightmare is daily reality.
But here’s the thing—technically, you can’t be allergic to water in the traditional sense. The human body is roughly 60% water, so a true allergic reaction would be incompatible with life. Yet this rare condition exists, and it’s as puzzling as it sounds.
What Is Aquagenic Urticaria?
Aquagenic urticaria is an extremely rare form of physical urticaria where skin contact with water triggers hives and intense itching. According to research published in medical literature, about 50 cases have been reported in the medical literature worldwide.
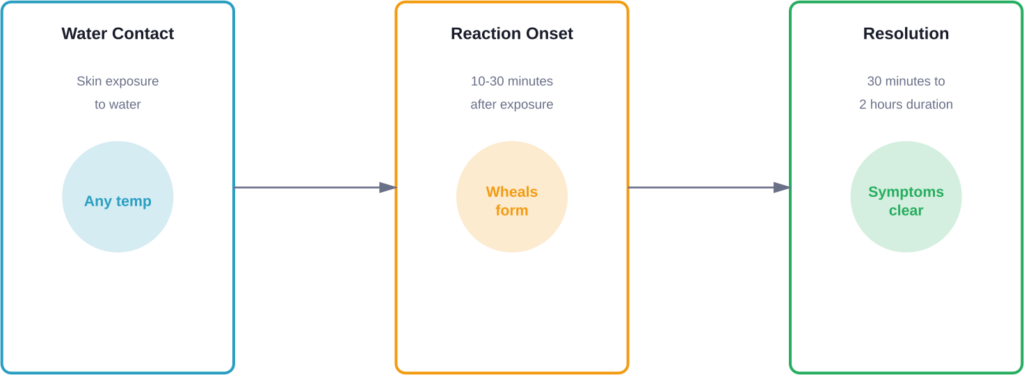
The condition causes small, folliculocentric wheals (1-3 mm) surrounded by larger areas of redness (1-3 cm flares) within 20-30 minutes of water exposure. These symptoms typically last between 30 minutes and 2 hours before resolving on their own.
What makes this condition particularly challenging is that it responds to water regardless of temperature or source. Hot water, cold water, saltwater, freshwater—it doesn’t matter. Even sweat and tears can trigger reactions in some patients.
Not Actually an Allergy
Despite being called a water allergy, aquagenic urticaria isn’t a true allergic reaction. Real allergies involve immunoglobulin E (IgE) antibodies responding to foreign proteins. Water is a simple molecule (H₂O) that can’t trigger this immune response.
The mechanism remains poorly understood. Current theories suggest the condition may result from:
- Interaction between water and specific compounds in or on the skin
- Release of histamine from mast cells triggered by water contact
- Sensitivity to substances dissolved in water that concentrate on the skin surface
- Changes in skin barrier function that allow water penetration into deeper skin layers
Recognizing the Symptoms
Symptoms of aquagenic urticaria develop rapidly after water contact. Most patients notice the reaction starting within 10-30 minutes of exposure.
The characteristic presentation includes the following features, typically appearing within 10-30 minutes of exposure:
- Small, pinpoint-sized wheals that resemble goosebumps
- Intense itching (pruritus) that can be severe
- Red, inflamed skin patches surrounding the wheals
- Burning or stinging sensations on the skin
- Symptoms affecting shoulders, arms, trunk, abdomen, and back most commonly
According to case reports in medical journals, episodes typically last 20-40 minutes before spontaneously resolving. However, some patients experience symptoms lasting up to 2 hours.
Extracutaneous Manifestations
While most symptoms affect the skin, some patients report additional complications. Research has documented cases with respiratory symptoms, digestive issues, and even systemic reactions in rare instances.
The difficulty of avoiding water entirely means patients face constant challenges. Showering, washing hands, sweating during exercise, or even walking in the rain can trigger reactions.
What Causes This Rare Condition?
The exact cause of aquagenic urticaria remains a mystery. Research hasn’t identified a single definitive trigger, though several theories exist.
One hypothesis suggests water interacts with sebum or other skin components to create a substance that releases histamine from mast cells. Another theory proposes that water itself causes physical changes in the skin barrier, leading to mast cell activation.
Some patterns have emerged from case studies:
- The condition often begins during or after puberty
- Females appear more commonly affected than males
- Family history may play a role, though cases are typically sporadic
- Some cases develop alongside other conditions like HIV infection or blood disorders
The condition appears to have both familial and acquired forms based on case reports. Familial cases run in families, while acquired cases develop spontaneously and represent the more common presentation.
Distinguishing From Aquagenic Pruritus
Aquagenic pruritus is a related but distinct condition. While aquagenic urticaria causes visible hives, aquagenic pruritus produces intense itching after water contact without any visible skin changes.
According to the Cleveland Clinic, aquagenic pruritus can start shortly after water contact and last from 10 minutes to 2 hours. It sometimes occurs as a symptom of other health conditions rather than as an independent disorder.
Diagnosis and Testing
Diagnosing aquagenic urticaria requires a combination of patient history and specialized testing. The wet towel provocation test serves as the diagnostic standard.
During this test, a clinician applies a water-soaked compress at body temperature (35°C) to the patient’s upper body for 30 minutes. A positive result shows the characteristic wheals and surrounding redness developing during or shortly after the test.
| Diagnostic Criteria | Details |
|---|---|
| Test Method | Wet towel provocation test |
| Water Temperature | Body temperature (35°C/95°F) |
| Application Duration | 30 minutes |
| Positive Result | 1-3 mm wheals with 1-3 cm erythema |
| Onset Time | During test or within 30 minutes after |
Doctors must rule out other conditions that might mimic aquagenic urticaria. These include cholinergic urticaria (triggered by body heat and sweating), cold urticaria (triggered by cold exposure), and various forms of contact dermatitis.
Treatment Options and Management
In chronic hives, doctors identify a cause in only about 10%-20% of cases, so treatment often focuses on managing symptoms rather than addressing an underlying trigger.
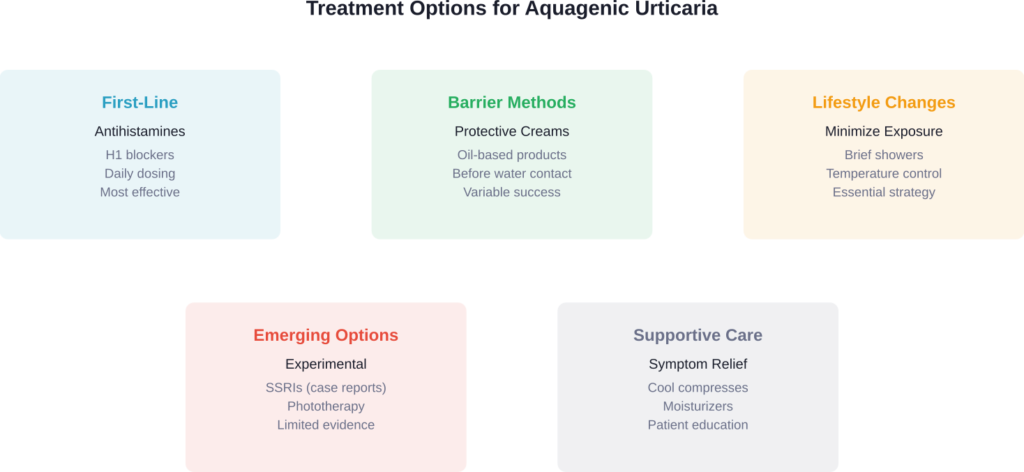
According to systematic reviews in medical literature, second-generation H1 antihistamines represent the recommended first-line treatment for both familial and acquired forms of aquagenic urticaria.
Common Treatment Approaches
Antihistamines help reduce the histamine release that causes wheals and itching. Case reports have documented successful management with:
- Desloratadine 5 mg once daily
- Ketotifen syrup for pediatric patients
- Dimetindene taken one hour before anticipated water contact
- Higher doses of standard antihistamines in resistant cases
Some patients achieve remission with consistent treatment, while others require ongoing medication management. The response varies considerably between individuals.
Barrier Methods
Patients have found creative ways to minimize water exposure and symptoms:
- Applying oil-based creams before showering to create a protective barrier
- Taking very brief showers (under 3 minutes)
- Using lukewarm rather than hot water, which some find less triggering
- Patting skin dry quickly rather than rubbing
- Wearing waterproof gloves for dishwashing and cleaning
Real talk: living with this condition requires significant lifestyle adjustments. Community discussions reveal that patients often feel isolated due to the rarity of their condition and the difficulty others have understanding it.
Living With Aquagenic Urticaria
The daily reality of this condition extends far beyond medical management. Patients face psychological and social challenges that can be profound.
Consider the basics most people take for granted. Showering becomes a calculated decision—is it worth the pain and itching? Exercising leads to sweat, which triggers symptoms. Rainy weather isn’t refreshing; it’s a hazard. Even crying during emotional moments causes physical distress.
One case featured Rachel Warwick, documented in a BBC article, whose own tears would cause burning pain on her face. She described drinking water as feeling like swallowing stinging nettles. The psychological impact of such constant vigilance can’t be understated.
Practical Coping Strategies
Patients and healthcare providers have developed various strategies to improve quality of life:
- Pre-medicating with antihistamines before necessary water exposure
- Scheduling showers strategically when time allows for recovery
- Keeping cool to minimize sweating
- Using fans and air conditioning liberally
- Wearing moisture-wicking fabrics
- Connecting with support communities online
The rarity of the condition means many patients initially struggle to get proper diagnosis and understanding from healthcare providers. Raising awareness remains crucial for improving outcomes.
Frequently Asked Questions
Aquagenic urticaria is not typically life-threatening. While the condition causes significant discomfort and impacts quality of life, the reactions are generally limited to the skin. Rare cases have reported extracutaneous manifestations, but severe systemic reactions are uncommon. The condition is manageable with proper medical care and lifestyle adjustments.
About 50 cases have been reported in the medical literature worldwide, making it exceptionally rare. The actual number of cases may be higher due to underdiagnosis or misdiagnosis, but it remains one of the rarest forms of physical urticaria. Most dermatologists may never encounter a case during their entire career.
Some cases have achieved remission with treatment, as documented in medical case reports. However, the condition is often chronic and requires ongoing management. Spontaneous resolution can occur, particularly in cases that began during adolescence, but this isn’t predictable. Most patients require long-term symptom management strategies.
Drinking water is essential and generally tolerable for most patients with aquagenic urticaria, though some report throat discomfort. The reaction primarily occurs with external skin contact rather than internal consumption. Patients do need to drink water to survive, and the internal exposure doesn’t typically trigger the same response as external contact.
The condition appears to have both familial and acquired forms. Familial aquagenic urticaria runs in families, suggesting a genetic component, though the specific genes involved haven’t been identified. Most cases are acquired rather than familial and develop spontaneously without family history. More research is needed to understand the genetic factors fully.
Aquagenic urticaria causes visible wheals and hives after water contact, while aquagenic pruritus produces intense itching without visible skin changes. Both conditions respond to water exposure, but the physical manifestation differs. Aquagenic pruritus may be associated with other underlying conditions, whereas aquagenic urticaria typically stands alone as a primary diagnosis.
Research remains limited due to the rarity of the condition. Case reports have documented experimental approaches including selective serotonin reuptake inhibitors for cases with extracutaneous manifestations, phototherapy, and various immunomodulating treatments. However, these treatments lack large-scale clinical trials, and antihistamines remain the evidence-based first-line approach.
The Bottom Line
So, is it possible to be allergic to water? Technically no—not in the traditional allergic sense. But aquagenic urticaria is very real and very challenging for those affected.
This rare condition demonstrates how much we still don’t understand about skin physiology and immune responses. With about 50 cases documented in the medical literature, research remains limited, and patients often navigate trial-and-error treatment approaches.
The condition isn’t life-threatening, but it significantly impacts daily life. Simple activities most people never think twice about require careful planning and often cause considerable distress.
If you experience hives or intense itching consistently after water contact, consult a dermatologist familiar with physical urticarias. The wet towel provocation test can confirm the diagnosis, and antihistamine therapy may provide relief.
For those living with aquagenic urticaria, connecting with support communities and working closely with knowledgeable healthcare providers makes a meaningful difference. While no cure exists yet, ongoing research continues to explore this fascinating and perplexing condition.