
Quick Summary: Yes, it’s absolutely possible to ovulate early—before day 14 of a menstrual cycle. According to the National Institutes of Health, the follicular phase typically ranges from 10 to 16 days, meaning ovulation can occur as early as day 8 or 9. Early ovulation doesn’t necessarily prevent pregnancy, but it can make timing conception more challenging if you’re tracking based on a standard 28-day cycle assumption.
The idea that everyone ovulates on day 14 of their cycle is one of the most persistent myths in reproductive health. Real talk: bodies don’t follow textbook timelines.
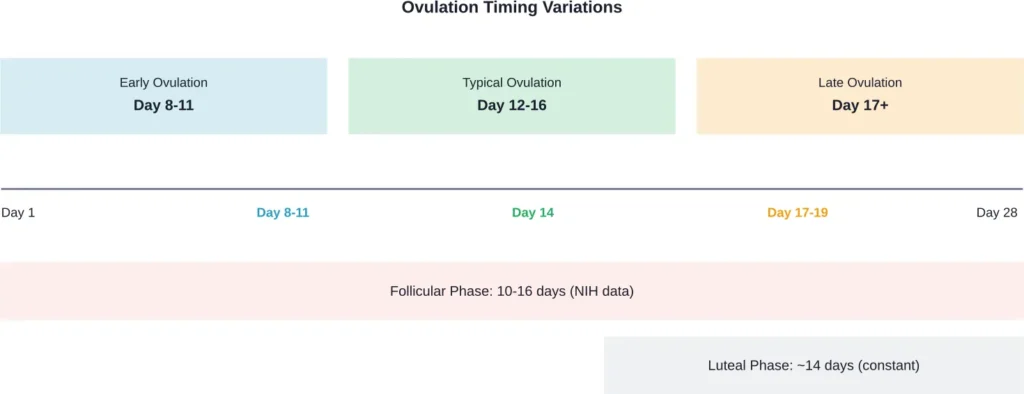
According to research published by the National Institutes of Health, while the luteal phase remains relatively constant at 14 days across most women, the follicular phase—the time from the first day of menstruation to ovulation—can range anywhere from 10 to 16 days. That means ovulation happening on day 8, 9, or 10 isn’t abnormal. It’s just variation.
But what causes this timing shift? Does it affect fertility or chances of conception? And more importantly, what can be done about it?
What Actually Counts as Early Ovulation?
Before diving into causes and solutions, it helps to establish what “early” actually means in this context.
Most fertility education operates on the assumption of a 28-day cycle with ovulation occurring around day 14. The truth? Only about 12.4% of women actually have cycles of exactly 28 days, with most people’s (87%) cycles falling between 23 and 35 days.
Early ovulation typically refers to ovulation that occurs before day 11 or 12 of the menstrual cycle. Some women ovulate as early as day 8 or 9, particularly those with shorter overall cycles of 21-24 days.
Here’s the thing though—early ovulation isn’t inherently problematic. The issue arises when timing doesn’t align with expectations, making it harder to predict the fertile window.
The Fertile Window Reality
According to the American College of Obstetricians and Gynecologists, the fertile window spans approximately 6 days each cycle. This window exists because sperm can survive in the reproductive tract for up to 5 days, while an egg remains viable for about 12 to 24 hours after ovulation.
When ovulation happens earlier than anticipated, couples trying to conceive might miss this narrow window entirely if they’re timing intercourse based on calendar methods that assume mid-cycle ovulation.
Why Does Early Ovulation Happen?
Several factors influence when ovulation occurs during a cycle. Some are temporary, others more persistent.
Shorter Follicular Phase
The NIH notes that cycle variability stems primarily from differences in the follicular phase—the period when follicles develop in the ovaries before releasing an egg. When this phase is shortened due to faster follicular development, ovulation naturally occurs sooner.
This isn’t necessarily dysfunction. It’s simply how some bodies operate.
Hormonal Fluctuations
The luteinizing hormone surge triggers ovulation. According to StatPearls, LH levels increase 10-fold during this surge, typically occurring 24-36 hours before the egg is released.
Certain conditions can cause this surge to happen earlier than expected. Stress, sleep disruption, and changes in exercise patterns can all influence the timing of hormone release.
Age-Related Changes
Research from the American College of Obstetricians and Gynecologists indicates that menstrual cycles tend to be most irregular around menarche (first period) and perimenopause. During perimenopause, which typically begins in the mid-40s, hormonal fluctuations can cause unpredictable ovulation timing, including earlier-than-usual ovulation.
Polycystic Ovary Syndrome and Other Conditions
While PCOS more commonly causes delayed or absent ovulation, research published in medical journals shows that premature LH surges can occur in women with PCOS undergoing fertility treatment, potentially disrupting the normal ovulation timeline.
Thyroid disorders, particularly hyperthyroidism, can also accelerate metabolic processes that affect cycle timing.
Lifestyle and Environmental Factors
The ACOG notes that environmental factors—including nutrition, stress levels, and access to healthcare—can influence both the timing and progression of reproductive events.
Sudden weight changes, intense exercise regimens, or significant stress events can temporarily shift ovulation timing earlier or later than baseline patterns.
Does Early Ovulation Affect Fertility?
This is where things get nuanced.
Early ovulation itself doesn’t necessarily reduce fertility. What matters more is the quality of the egg released and whether the fertile window can be accurately identified.
Egg Quality Considerations
Some research suggests that when follicular development is significantly compressed, there might be concerns about egg maturation. However, many women who ovulate early conceive without difficulty.
The more pressing issue? Timing intercourse appropriately.
The Timing Challenge
According to the CDC, the Standard Days Method of fertility awareness assumes fertility occurs on days 8-19 of the cycle. For someone who ovulates on day 9, this method might just barely capture the fertile window—but it wouldn’t work at all for someone ovulating on day 8.
Community discussions on platforms frequented by couples trying to conceive reveal a common frustration: discovering ovulation happened much earlier than expected, meaning intercourse timing was off by several days.
Short Cycles and Luteal Phase Length
Here’s what really matters: the luteal phase length. This is the time between ovulation and the next period.
According to NIH research, the luteal phase should be approximately 14 days. If early ovulation is part of a very short cycle (say, 21 days) with a shortened luteal phase (10 days or less), this could indicate luteal phase deficiency—a condition that may affect embryo implantation.
But if early ovulation occurs with a normal 14-day luteal phase, fertility potential remains intact.
| Cycle Pattern | Ovulation Day | Luteal Phase | Fertility Impact |
|---|---|---|---|
| Standard cycle | Day 14 | 14 days | Normal |
| Early ovulation, normal luteal | Day 10 | 14 days | Normal (timing challenge only) |
| Early ovulation, short luteal | Day 9 | 10 days | May reduce implantation success |
| Very short cycle | Day 8 | 11 days | Possible luteal deficiency |
How to Identify Early Ovulation
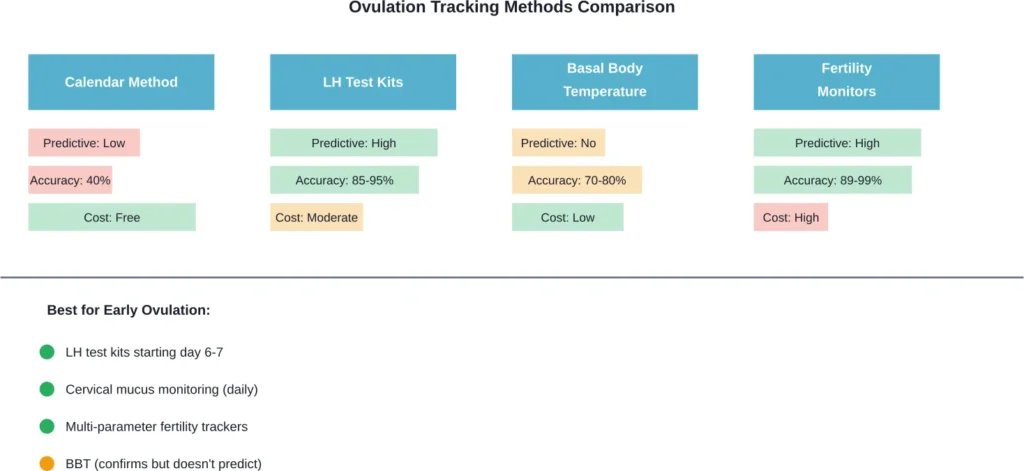
Calendar-based predictions fall short when cycle timing varies. More precise tracking methods provide better data.
Ovulation Predictor Kits
These kits detect the LH surge in urine. Since LH rises 24-36 hours before ovulation, a positive test indicates ovulation is imminent.
For those with early ovulation, starting testing around day 6 or 7 of the cycle (rather than the typical day 10-11) prevents missing the surge entirely.
Basal Body Temperature Tracking
According to StatPearls, basal body temperature—the lowest natural body temperature at rest—shifts after ovulation due to progesterone. Consistent morning measurements can confirm ovulation occurred, though they don’t predict it in advance.
One commercially available vaginal temperature sensor demonstrates 89% accuracy in predicting ovulation, offering more precision than manual oral temperature tracking.
Cervical Mucus Monitoring
As ovulation approaches, cervical mucus changes from thick and sticky to clear, slippery, and stretchy—often compared to raw egg whites. This change signals peak fertility.
Observing these changes provides real-time information regardless of when ovulation occurs in the cycle.
Fertility Tracking Apps and Wearables
Research analyzing data from self-tracking health apps reveals significant variation in ovulation timing across users. Modern fertility apps that incorporate multiple data inputs—basal temperature, LH tests, cervical mucus observations—provide more accurate predictions than calendar methods alone.
What Can Be Done About Early Ovulation?
The approach depends on whether early ovulation is causing problems.
When Early Ovulation Isn’t a Problem
If cycles are consistent (even if short), the luteal phase is adequate, and conception goals are being met—or if pregnancy isn’t currently a goal—early ovulation requires no intervention.
Awareness and appropriate tracking are sufficient.
Addressing Luteal Phase Deficiency
When early ovulation accompanies a shortened luteal phase (less than 10-11 days), medical evaluation makes sense. Progesterone supplementation during the luteal phase may help support implantation, though research on its effectiveness remains mixed.
Managing Underlying Conditions
If thyroid dysfunction, PCOS, or other hormonal imbalances are identified, treating the underlying condition often normalizes cycle timing.
Thyroid medication, insulin-sensitizing drugs for PCOS, or other targeted treatments address root causes rather than symptoms.
Lifestyle Modifications
While lifestyle factors alone rarely cause persistent early ovulation, optimizing sleep patterns, managing stress, maintaining stable body weight, and moderating intense exercise can help stabilize cycle timing.
Nutritional support—particularly adequate caloric intake and micronutrients like vitamin D, B vitamins, and omega-3 fatty acids—supports overall reproductive health.
Assisted Reproductive Technology Considerations
For couples pursuing fertility treatment, early ovulation or premature LH surges can complicate ovarian stimulation protocols. Research indicates that close monitoring and protocol adjustments can mitigate these challenges.
When to See a Healthcare Provider
Not every instance of early ovulation requires medical attention. But certain scenarios warrant consultation.
According to CDC data, about 19% of married women aged 15-49 with no prior births are unable to get pregnant after one year of trying. If early ovulation is suspected and conception hasn’t occurred after 6-12 months of appropriately timed intercourse, evaluation is appropriate.
Other red flags include:
- Cycles consistently shorter than 21 days
- Luteal phases shorter than 10 days
- Significant cycle irregularity or unpredictability
- Accompanying symptoms like excessive hair growth, severe acne, or significant weight changes
- Age over 35 and trying to conceive for more than 6 months
A reproductive endocrinologist or fertility specialist can perform hormone testing, ultrasound monitoring, and other diagnostics to identify treatable issues.
The Bottom Line on Early Ovulation
Yes, early ovulation is possible—and more common than standard fertility education suggests.
The NIH data is clear: follicular phase length varies significantly, and ovulation can occur anywhere from day 8 to day 20 or later in a normal, healthy cycle. The assumption that ovulation always happens on day 14 reflects averages, not individual biology.
For most individuals, early ovulation poses no inherent fertility problem. The challenge lies in accurate identification of the fertile window. With appropriate tracking methods—particularly LH testing started earlier in the cycle and cervical mucus monitoring—timing intercourse becomes straightforward regardless of when ovulation occurs.
The more important factor is luteal phase adequacy. As long as the post-ovulation phase lasts approximately 14 days, egg quality is adequate, and no underlying medical conditions exist, early ovulation is simply a variation of normal.
That said, if early ovulation accompanies very short cycles, luteal phase deficiency, or difficulty conceiving, medical evaluation can identify and address potential issues.
Frequently Asked Questions
Absolutely. Early ovulation doesn’t prevent pregnancy—it just changes when the fertile window occurs. According to ACOG, the fertile window spans about 6 days, ending on ovulation day. If intercourse timing aligns with this window regardless of when it falls in the cycle, conception is possible. The key is identifying when ovulation actually happens rather than relying on calendar-based assumptions.
Based on NIH research showing follicular phases can be as short as 10 days, ovulation can occur as early as day 8 or 9 of a menstrual cycle in some women. While less common, day 7 ovulation is physiologically possible in very short cycles. These early ovulations are more likely to occur in women with naturally shorter cycles of 21-24 days.
Not necessarily. While some research suggests that very compressed follicular development might theoretically affect egg maturation, many women who ovulate early conceive healthy pregnancies. The more relevant concern is whether the luteal phase is adequate (approximately 14 days) and whether any underlying hormonal imbalances exist. Early ovulation with normal hormonal patterns typically doesn’t indicate egg quality issues.
Start ovulation predictor kit testing around day 6 or 7 of your cycle rather than the typical day 10-11 recommendation. Monitor cervical mucus changes daily starting right after menstruation ends. Consider using a fertility tracking app that incorporates multiple data points rather than relying solely on calendar predictions. Basal body temperature tracking can confirm ovulation occurred but won’t predict it in advance.
Stress can influence ovulation timing, though research shows it more commonly delays ovulation rather than advancing it. However, significant stress, sleep disruption, or lifestyle changes can alter the hormonal patterns that regulate the menstrual cycle. While isolated stressful events might shift timing temporarily, persistent early ovulation usually relates to individual cycle characteristics rather than stress alone.
It can be. The ACOG notes that cycles tend to be most irregular during perimenopause, typically beginning in the mid-40s, with unpredictable ovulation timing including both early and late ovulation. However, early ovulation alone isn’t definitive evidence of perimenopause—particularly in younger women. Other perimenopausal signs include cycle length changes, hot flashes, sleep disturbances, and mood changes.
If cycles are consistent, the luteal phase is adequate (about 14 days from ovulation to next period), and no conception difficulties exist, early ovulation typically doesn’t require medical intervention. However, consult a healthcare provider if cycles are consistently shorter than 21 days, luteal phases are less than 10 days, conception hasn’t occurred after 6-12 months of appropriately timed intercourse, or other concerning symptoms are present. According to CDC data, fertility evaluation is recommended after one year of trying for women under 35, or six months for women over 35.
Moving Forward
Understanding personal cycle patterns matters more than conforming to textbook averages.
Early ovulation isn’t a disorder to be fixed unless it’s accompanied by luteal phase inadequacy or other hormonal imbalances. For most people, it’s simply a matter of accurate tracking and appropriate timing.
The tools exist to identify ovulation regardless of when it occurs. LH tests, cervical mucus observation, and modern fertility monitors provide data that calendar methods can’t match.
If early ovulation is making conception challenging, or if questions about cycle health arise, consultation with a reproductive specialist provides clarity. Hormone testing and ultrasound monitoring can reveal whether any intervention is beneficial.
But for those whose cycles run on the early side? Know that it’s variation, not dysfunction—and with proper awareness, it doesn’t have to be an obstacle.