
Quick Summary: Yes, it’s possible to not ovulate—a condition called anovulation that affects approximately one in ten women of childbearing age. While you may still experience bleeding that resembles a period, no egg is released, making pregnancy impossible during that cycle. Anovulation can be temporary or chronic, with causes ranging from polycystic ovary syndrome (PCOS) to stress, weight changes, and hormonal imbalances.
Most women assume that having a period automatically means ovulation happened. That’s not always true.
Anovulation—when your ovaries don’t release an egg during a menstrual cycle—is far more common than most people realize. According to research cited by fertility centers, approximately one in ten women of childbearing age experiences anovulation. And here’s what catches many off guard: you can still bleed regularly without ovulating at all.
This matters especially if you’re trying to conceive, tracking your cycle for health insights, or wondering why conception isn’t happening despite regular periods. Understanding whether you’re actually ovulating each month can explain fertility challenges, irregular symptoms, and underlying health conditions that need attention.
What Exactly Is Anovulation?
Anovulation means your ovaries fail to release an egg during a menstrual cycle. No egg release means no possibility of pregnancy during that cycle, regardless of when or how often intercourse occurs.
But here’s where it gets confusing: anovulation doesn’t always mean your period stops. Many women with anovulation still experience bleeding—sometimes heavy, sometimes irregular—that looks like a normal period. The difference? That bleeding comes from hormonal fluctuations and uterine lining shedding without the progesterone surge that follows actual ovulation.
Medical research published in the NIH’s StatPearls defines this as abnormal uterine bleeding associated with ovulatory dysfunction (AUB-O). The annual rate of abnormal uterine bleeding (AUB) in the United States has been reported at 53 per 1000 reproductive-aged women, with anovulation identified as a leading cause once regular menstruation is established.
When Anovulation Is Normal
Not all anovulation signals a problem. According to research in the BMJ, anovulatory cycles are physiological during specific life stages:
- Puberty and the first few years after menarche
- Postpartum period, especially while breastfeeding
- Perimenopause (the transition before menopause)
During these phases, your body’s hormonal systems are either developing, recovering, or winding down reproductive function. Occasional anovulatory cycles can happen to healthy women too—research shows that even women with generally regular cycles may experience sporadic anovulation.
Why Anovulation Happens: The Primary Causes
When anovulation becomes chronic or happens during reproductive years outside normal physiological windows, underlying causes need investigation.
Polycystic Ovary Syndrome (PCOS)
PCOS stands as the heavyweight champion of anovulation causes. According to the World Health Organization, PCOS is the most common cause of anovulatory infertility globally, affecting an estimated 10-13% of reproductive-aged women. Some estimates suggest up to 70% of women with PCOS worldwide don’t know they have the condition.
The BMJ notes that PCOS causes approximately 70% of anovulatory subfertility cases. The condition creates excess androgens and insulin resistance, disrupting the normal follicle development needed for ovulation. Follicles arrest at 5-10mm instead of maturing to release an egg.
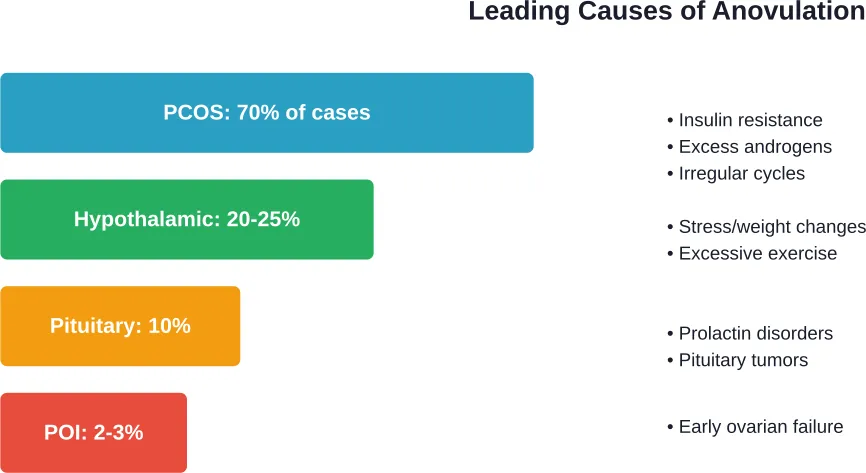
Hypothalamic Dysfunction
The hypothalamus controls hormone release that triggers ovulation. When this system malfunctions, ovulation stops. Common triggers include:
- Significant weight loss or low body weight (BMI below 18.5)
- Excessive exercise (common in athletes)
- Chronic stress
- Eating disorders
Research published in Reproduction and Fertility journal examined athletes specifically. The study found that 26% of athletic women sampled failed to reach progesterone levels of 16 nmol/L during the mid-luteal phase—the threshold for confirming ovulation. These women exhibited anovulatory cycles or cycles with deficient luteal phases.
Thyroid Disorders
According to the Office on Women’s Health, women are more likely than men to have thyroid diseases, especially after pregnancy and menopause. Both hyperthyroidism (overactive thyroid) and hypothyroidism (underactive thyroid) can disrupt ovulation.
Postpartum thyroiditis, or inflammation of the thyroid after giving birth, affects 10% of women, often causing symptoms mistaken for normal postpartum fatigue and mood changes.
Premature Ovarian Insufficiency (POI)
POI occurs when ovaries stop functioning normally before age 40. The condition affects approximately 1% of women under 40 and causes irregular or absent ovulation despite younger age. The American College of Obstetricians and Gynecologists notes that women with POI have only modest odds of spontaneous pregnancy.
Recognizing the Signs You’re Not Ovulating
Anovulation doesn’t always announce itself clearly. Some women have obvious symptoms; others have subtle changes easily dismissed.
| Symptom Category | What to Watch For | Why It Matters |
|---|---|---|
| Menstrual Irregularity | Cycles shorter than 21 days or longer than 35 days; unpredictable timing | Regular ovulation typically produces consistent 25-35 day cycles |
| Absent Periods | Missing periods for 3+ months (excluding pregnancy) | Amenorrhea happens in 3% to 4% of women and often indicates anovulation |
| Abnormal Bleeding | Very heavy, prolonged, or very light periods | Without progesterone from ovulation, bleeding patterns become erratic |
| Missing Ovulation Signs | No cervical mucus changes, no mittelschmerz (ovulation pain), flat BBT chart | Ovulation produces detectable physical changes; absence suggests anovulation |
| Difficulty Conceiving | 12+ months trying without pregnancy (or 6+ months if over 35) | Anovulation causes approximately 30% of fertility problems |
The Cervical Mucus Clue
One of the most reliable home indicators is cervical mucus. Around ovulation, rising estrogen produces clear, stretchy, egg-white consistency mucus. Without ovulation, this characteristic change doesn’t occur. Many women with anovulation report minimal mucus changes throughout their cycle.
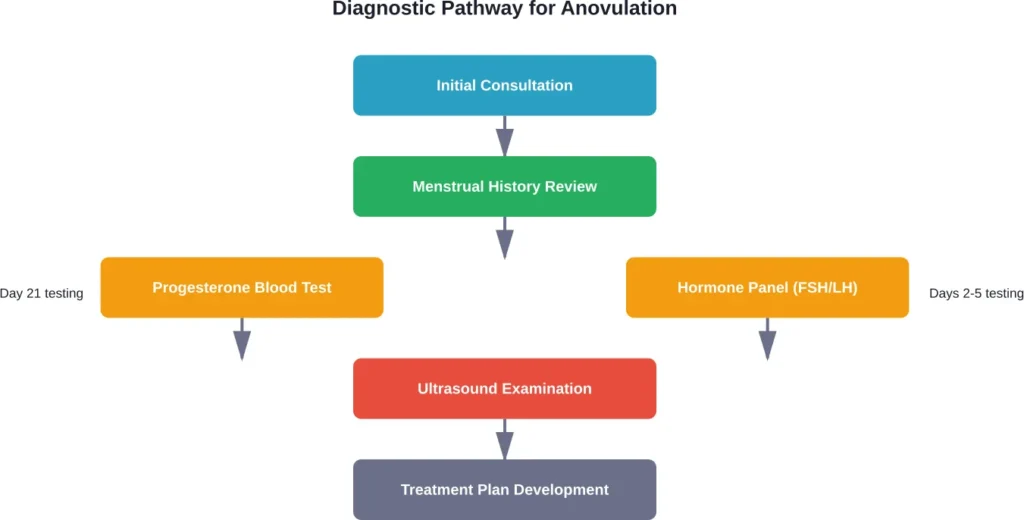
How Doctors Diagnose Anovulation
Self-observation provides clues, but medical testing confirms anovulation definitively.
Progesterone Testing
This is the gold standard. Research defines ovulatory cycles as those reaching progesterone levels of at least 16 nmol/L during the mid-luteal phase. Anovulation has been defined in studies as peak serum progesterone concentrations ≤5 ng/ml and no serum LH peak detected during the mid- or late-luteal phase.
Testing typically happens 7 days before expected menstruation (around day 21 in a 28-day cycle). Low progesterone confirms no ovulation occurred.
Additional Diagnostic Tools
- LH testing: Ovulation predictor kits detect the LH surge that triggers ovulation. Absent surges suggest anovulation.
- Ultrasound: Transvaginal ultrasound tracks follicle development and can identify conditions like PCOS.
- Hormone panels: FSH, estradiol, thyroid hormones, and prolactin levels reveal underlying causes.
- AMH testing: Anti-Müllerian hormone indicates ovarian reserve and helps diagnose conditions like PCOS.
Treatment Options That Actually Work
Treatment depends entirely on the underlying cause and whether fertility is currently a goal.
Lifestyle Modifications
For hypothalamic anovulation related to weight or exercise, lifestyle changes often restore ovulation without medication. Research shows body mass index outside the 18.5-30 range increases anovulation risk significantly. Achieving healthy weight through balanced nutrition frequently resolves the issue.
Athletes may need to reduce training intensity or increase caloric intake to restore normal hormonal function.
Ovulation Induction Medications
For women actively trying to conceive, ovulation induction represents first-line medical treatment.
Clomiphene citrate: According to WebMD, approximately 80% of women who take clomiphene citrate will ovulate, and approximately 40% will become pregnant. The BMJ confirms clomiphene remains the first-line treatment for inducing ovulation in PCOS-related anovulation.
Letrozole: Originally a breast cancer medication, letrozole has become a preferred ovulation induction agent for PCOS patients, often showing better outcomes than clomiphene for this population.
Gonadotropins: Injectable hormones (FSH and LH) directly stimulate follicle development when oral medications fail. The BMJ notes these treatments require careful monitoring to reduce multiple pregnancy risks.
Treating Underlying Conditions
| Condition | Primary Treatment | Expected Outcome |
|---|---|---|
| PCOS | Metformin, lifestyle changes, ovulation induction | Restored ovulation in 60-70% with combined approach |
| Hypothyroidism | Levothyroxine replacement | Normal ovulation typically returns with proper dosing |
| Hyperprolactinemia | Dopamine agonists (cabergoline, bromocriptine) | High success rate for normalizing prolactin and restoring cycles |
| Premature Ovarian Insufficiency | Hormone replacement therapy; donor eggs for fertility | Spontaneous ovulation possible but unpredictable |
Assisted Reproductive Technology
When medication-induced ovulation fails or other factors complicate fertility, intrauterine insemination (IUI) or in vitro fertilization (IVF) become options. Fertility centers report that combining ovulation induction with timed IUI improves conception rates beyond medication alone.
When to See a Doctor
Timing matters for evaluation. Consider medical consultation if:
- You’ve been trying to conceive for 12+ months without success (or 6+ months if over age 35)
- Your periods come fewer than 8 times yearly
- Periods stopped for 3+ months outside of pregnancy
- Cycles consistently fall outside the 21-35 day range
- You’re experiencing symptoms of hormonal imbalance (excessive hair growth, severe acne, significant weight changes)
The Office on Women’s Health notes that 3-4% of women experience amenorrhea, and early evaluation prevents complications and identifies treatable conditions before they impact long-term health.
But here’s something not enough doctors mention: even if you’re not currently trying to conceive, chronic anovulation matters for bone health, cardiovascular risk, and endometrial cancer risk. Anovulation means low progesterone, which over years can cause problems beyond fertility.
Living With Anovulation: What to Know
For women not immediately seeking pregnancy, managing anovulation focuses on long-term health protection. Combined hormonal contraceptives can regulate bleeding patterns and protect the endometrium from unopposed estrogen exposure.
Regular monitoring becomes important. Annual checkups should include discussion of menstrual patterns, and any significant changes warrant evaluation.
Frequently Asked Questions
No. Pregnancy requires an egg to be released and fertilized. Without ovulation, no egg is available for fertilization, making conception impossible during that specific cycle. However, anovulation can be intermittent—some cycles may be anovulatory while others aren’t.
Yes. Anovulatory bleeding occurs when hormonal fluctuations cause the uterine lining to shed without prior ovulation. This bleeding can look identical to a regular period but lacks the progesterone surge that follows true ovulation. Many women with anovulation still experience monthly bleeding.
In research studies, anovulation has been identified in 3.4% to 18.6% of menstruating women, depending on the diagnostic criteria used. Even women with generally regular cycles may have occasional anovulatory cycles. Studies show that sporadic anovulation can occur in otherwise healthy premenopausal women without indicating disease.
Not necessarily. While PCOS causes approximately 70% of anovulatory infertility cases according to BMJ research, many other conditions cause anovulation including thyroid disorders, stress, weight changes, excessive exercise, and pituitary problems. Proper diagnosis requires medical evaluation beyond just identifying absent ovulation.
If hypothalamic dysfunction or PCOS related to weight is causing anovulation, achieving healthy weight often restores ovulation. Research indicates BMI outside the 18.5-30 range significantly increases anovulation risk. For PCOS specifically, losing 5-10% of body weight can improve hormonal balance and restore regular ovulation in many cases.
Yes. Chronic stress affects the hypothalamic-pituitary-ovarian axis that controls ovulation. Severe or prolonged stress can suppress GnRH (gonadotropin-releasing hormone) release from the hypothalamus, preventing the hormone cascade needed for follicle development and ovulation. This represents a form of hypothalamic anovulation.
This varies by cause and treatment. For lifestyle-related anovulation, changes may restore ovulation within 2-6 months. Medications like clomiphene typically work within the first treatment cycle if they’re going to be effective. Treating underlying conditions like thyroid disorders may take several months of optimized medication dosing before ovulation normalizes.
Bottom Line
Anovulation—not ovulating during a menstrual cycle—is both possible and surprisingly common, affecting approximately one in ten women of reproductive age. You can experience what seems like regular periods while not ovulating at all, since anovulatory bleeding mimics true menstruation.
The condition matters whether fertility is an immediate concern or not. Chronic anovulation causes roughly 30% of fertility problems, but it also affects long-term bone health, cardiovascular risk, and endometrial cancer risk through prolonged low progesterone exposure.
Medical science offers effective solutions. From lifestyle modifications that restore natural ovulation to proven medications like clomiphene citrate (which induces ovulation in 80% of users), most women with anovulation can achieve successful treatment. The critical step is identifying the underlying cause through proper medical evaluation.
If your cycles are irregular, you’ve been trying to conceive without success for over a year, or you suspect hormonal imbalance, consult a healthcare provider. Testing is straightforward, causes are usually identifiable, and treatment restores not just fertility potential but overall reproductive health.