
Quick Summary: It is extremely rare to vomit while fully asleep without waking up due to protective airway reflexes that automatically trigger awakening. However, certain conditions like severe neurological disorders, heavy sedation, or impaired reflexes can increase aspiration risk. Most people wake seconds before or during vomiting, even if they don’t fully remember it.
The fear of vomiting while unconscious keeps many people awake when they’re feeling nauseous. Whether you’re trying to sleep off food poisoning or dealing with chronic nighttime nausea, the question haunts you: could your body actually throw up without waking you?
The short answer? It’s incredibly unlikely in healthy individuals. But the mechanisms behind this protection—and the exceptions—are more complex than most people realize.
Understanding how the body defends the airway during sleep matters for anyone experiencing nocturnal nausea, caring for someone who’s ill, or managing conditions that increase aspiration risk.
How Your Body Protects Against Aspiration During Sleep
The human body has evolved sophisticated protective mechanisms specifically designed to prevent dangerous substances from entering the lungs. These reflexes remain active even during sleep, though they function differently than when fully conscious.
The Laryngeal Chemoreflex and Airway Protection
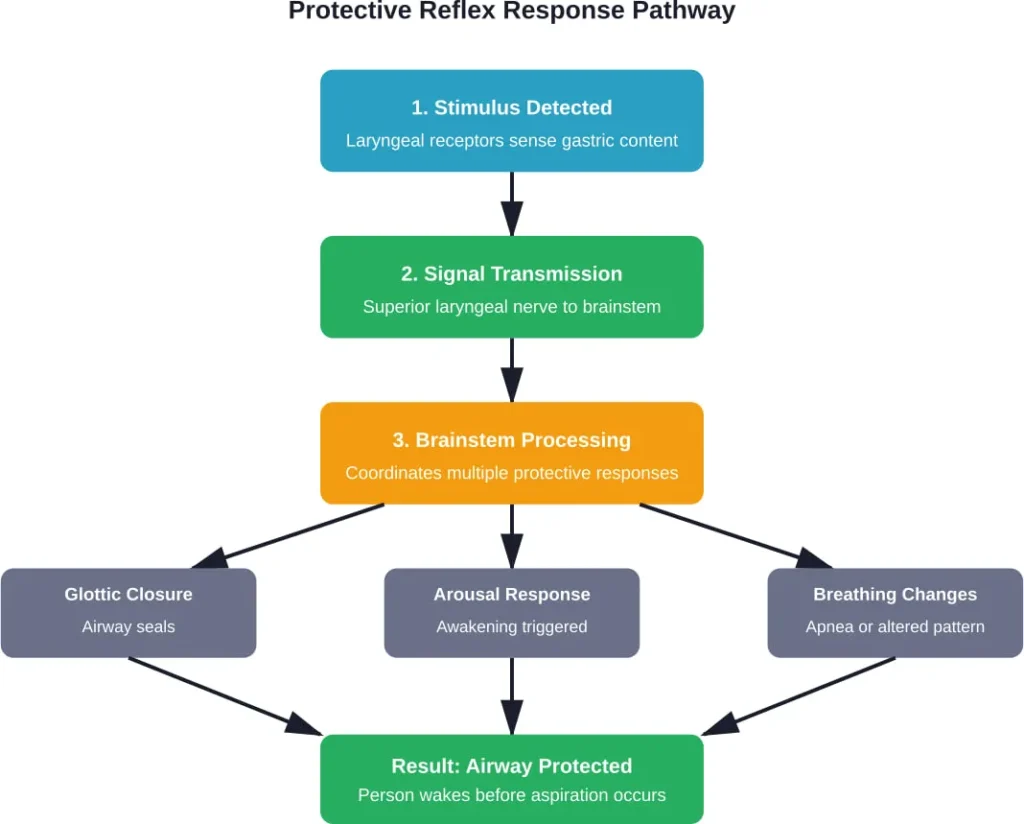
According to research published in Chemical Senses, the laryngeal chemoreflex serves as a primary defense mechanism. When the larynx detects potentially harmful substances—whether liquid, particulate matter, or gastric content—it triggers an immediate protective response.
This reflex operates on multiple levels simultaneously. The glottis closes rapidly, breathing patterns change, and most importantly for sleep safety, arousal mechanisms activate.
These aerodigestive reflexes work in coordination. Research from the Medical College of Wisconsin found that the hypopharynx can safely hold a small volume of liquid (colored water was perfused at 1 mL/min in studies) before protective mechanisms kick in. Once threshold volumes are exceeded, the pharyngoglottal closure reflex activates automatically.
Here’s what actually happens: sensory nerves in the supraglottis and glottis detect chemical changes or mechanical stimulation. Signals travel through the superior laryngeal nerve to the brainstem. The brainstem then coordinates a multi-system response that almost always includes awakening.
Why Sleep Doesn’t Turn Off Protective Reflexes
Sleep stages affect reflex sensitivity, but they don’t eliminate protection entirely. During lighter sleep stages, reflexes respond nearly as quickly as during wakefulness. Even in deeper sleep, sufficient stimulation—like stomach contents moving toward the throat—triggers arousal.
The esophagoglottal closure reflex, as documented by researchers at Ohio State University, remains functional across sleep stages. When esophageal peristalsis moves content upward, glottal responses correlate with the stimulus volume and type.
But there’s a critical point here: these reflexes depend on intact neurological function and normal anatomy. When those conditions aren’t met, protection breaks down.
Can You Actually Vomit While Fully Asleep?
The medical consensus is clear: true vomiting while completely unconscious is exceptionally rare in people with normal neurological function. Most reported cases of “vomiting in sleep” involve partial arousal that the person doesn’t remember.
What the Research Shows
According to research published in Gastroenterology, protective reflexes remain robust even under challenging conditions. Studies using pharyngeal perfusion found that healthy subjects consistently demonstrate arousal responses when liquid volumes exceed safe thresholds.
The Agency for Healthcare Research and Quality documented a case where aspiration occurred during medical sedation—but this involved pharmacological suppression of protective reflexes, not natural sleep. The case involved a patient undergoing endoscopy who experienced aspiration resulting in cardiac arrest.
That distinction matters. Medical sedation actively suppresses the reflexes that natural sleep preserves.
The Exception Cases
Certain conditions do increase aspiration risk during sleep. According to StatPearls, these include:
- Advanced cerebrovascular disease affecting brainstem function
- Severe neurological disorders that impair reflex pathways
- Altered mental status from head trauma or metabolic derangements
- Esophageal motility disorders that prevent normal clearance
- Persistent vomiting that exhausts protective mechanisms
- Gastric outlet obstruction causing overwhelming reflux volume
Heavy alcohol intoxication or drug overdose also impairs protective reflexes. This is why positioning matters so critically in emergency situations—the reflexes that normally trigger awakening may be chemically suppressed.
But for someone dealing with garden-variety nausea while sober? The body’s protective systems work remarkably well.
Why You Wake Up Nauseous or Vomiting at Night
Waking up already feeling sick—or waking in the act of vomiting—creates confusion. What happened during sleep to trigger this?
Generally speaking, nighttime nausea has distinct causes compared to daytime queasiness. The horizontal position, prolonged fasting, and circadian effects on digestive function all play roles.
Gastroesophageal Reflux Disease
GERD ranks among the most common causes of nocturnal nausea and vomiting. Acid reflux events occur frequently during sleep, and research indicates that conscious awakenings are commonly associated with acid reflux events.
The mechanism is straightforward: lying flat eliminates gravity’s assistance in keeping stomach contents down. When the lower esophageal sphincter relaxes inappropriately, acid moves upward. This triggers both the burning sensation and nausea.
Interestingly, research indicates that shorter dinner-to-bed intervals significantly increase reflux risk. Eating within two to three hours of sleep gives the stomach less time to empty.
Sleep deprivation has been shown to worsen pain perception in patients with GERD, potentially explaining why symptoms feel worse on nights with poor sleep quality.
Peptic Ulcers and Gastritis
Stomach ulcers often cause pain and nausea that peaks during fasting periods. Since most people go eight to twelve hours without eating during sleep, the overnight fast can trigger significant discomfort.
The stomach produces acid continuously, but food buffers this acid during waking hours. At night, acid accumulates and can irritate ulcerated areas, triggering nausea severe enough to cause awakening.
Low Blood Sugar
Hypoglycemia represents another nighttime culprit. Low blood sugar levels can result in weakness, dizziness, and nausea. For some people, particularly those with diabetes or other metabolic conditions, the overnight fast produces significant blood sugar drops.
When blood glucose falls below normal thresholds, counter-regulatory hormones release. This hormonal response can trigger nausea as a side effect.
Gastroparesis
Delayed gastric emptying causes food to remain in the stomach far longer than normal. Meals eaten at dinner may still be partially undigested at bedtime, creating persistent fullness and nausea.
The horizontal sleeping position can worsen symptoms by reducing what little gastric motility remains. This condition commonly affects people with diabetes or following certain surgeries.
Pregnancy-Related Nausea
Morning sickness is misleadingly named—it strikes at any hour. Hormonal fluctuations during pregnancy affect the entire day, and many women find symptoms particularly troublesome upon waking or during the night.
The extended fasting period during sleep may worsen pregnancy nausea. Empty stomach + hormonal changes = significant discomfort for many expectant mothers.
Medications and Side Effects
Many medications cause nausea as a side effect, particularly when taken on an empty stomach. Since most people go eight to twelve hours without eating while asleep, morning represents the peak fasting period.
Medications taken at bedtime may produce nausea that manifests hours later, causing middle-of-the-night or early morning awakening.
Anxiety and Stress Disorders
Psychological factors significantly influence nighttime nausea. Anxiety disorders often cause physical symptoms including digestive disturbances. Some people experience anticipatory nausea about the coming day, which manifests as early morning stomach upset.
The connection between mental health and gastrointestinal function runs deep. Stress affects gut motility, acid production, and visceral sensitivity.
| Condition | Primary Mechanism | Timing Pattern | Key Identifying Features |
|---|---|---|---|
| GERD | Acid reflux into esophagus | 1-3 hours after lying down | Burning sensation, sour taste, worse after large meals |
| Peptic Ulcer | Acid irritation of ulcerated tissue | Peak during fasting periods | Epigastric pain, relief with food or antacids |
| Gastroparesis | Delayed stomach emptying | Several hours post-meal | Early satiety, bloating, feeling full from dinner |
| Low Blood Sugar | Hypoglycemia triggers hormones | Early morning hours | Shakiness, sweating, confusion, improves with eating |
| Pregnancy | Hormonal fluctuations | Upon waking or any time | Missed period, other pregnancy signs |
| Medication Side Effects | Direct gastric irritation or CNS effects | Related to dosing schedule | Correlation with new medications or dose changes |
Understanding Aspiration Pneumonia Risk
When vomit does enter the lungs—whether during sleep or wakefulness—aspiration pneumonia becomes a serious concern. According to StatPearls, this infectious pulmonary condition results from bacteria-rich oropharyngeal fluids entering the lower respiratory tract.
Aspiration pneumonia affects primarily older adults and those with specific risk factors. The condition carries significant morbidity and mortality risks, particularly among individuals with neurological disorders or swallowing difficulties.
Who’s Actually at Risk?
StatPearls identifies several high-risk groups:
- Advanced age (physiological changes reduce protective reflex sensitivity)
- Cerebrovascular disease affecting swallowing coordination
- Neurological conditions impairing consciousness or motor control
- Esophageal motility disorders preventing normal clearance
- Individuals with learning disabilities affecting swallowing mechanics
- Those experiencing persistent vomiting that exhausts defenses
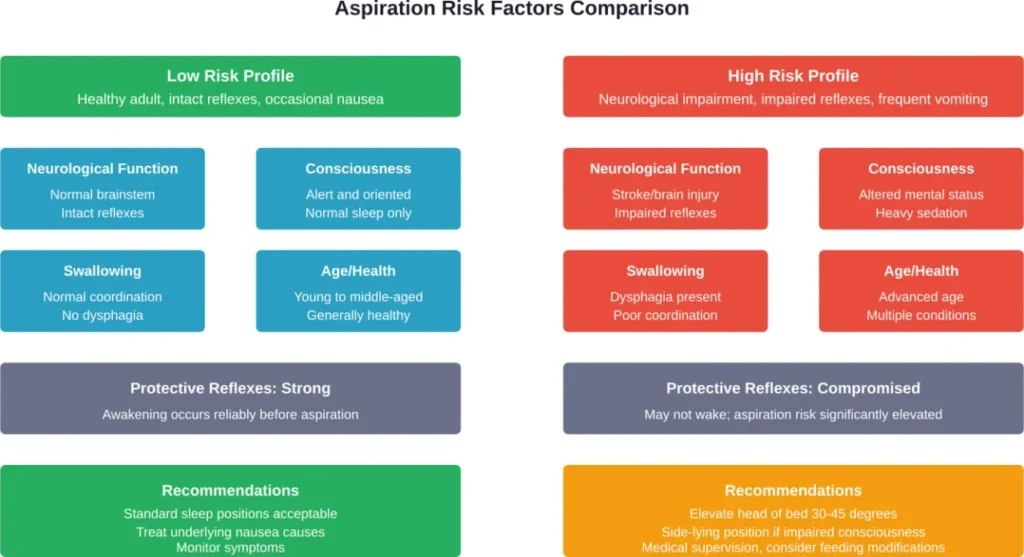
The risk isn’t equally distributed. A healthy young adult experiencing occasional nighttime nausea faces minimal aspiration risk. An elderly stroke patient with dysphagia faces substantially elevated risk.
Prevention for High-Risk Individuals
For those caring for someone with elevated aspiration risk, positioning matters tremendously. Elevating the head of the bed reduces reflux and makes aspiration mechanically more difficult.
Medical professionals recommend side-lying positions for individuals with impaired consciousness or protective reflexes. This position allows fluids to drain from the mouth rather than pooling in the throat.
Timing of meals also plays a role. Avoiding food for at least three hours before bedtime gives the stomach time to empty, reducing the volume of potential aspirate.
What to Do When Nausea Strikes at Night
Managing nighttime nausea effectively reduces both discomfort and any minimal aspiration risk. Practical strategies make a significant difference.
Immediate Relief Measures
When nausea wakes someone at night, position changes often provide quick relief. Sitting upright or propping up with pillows reduces reflux and often eases stomach discomfort.
Cool air can help. Opening a window or using a fan provides fresh air that many people find reduces nausea intensity.
Sipping small amounts of water or clear fluids helps, though large volumes can worsen symptoms. Room-temperature or slightly cool liquids tend to work best.
Dietary and Lifestyle Modifications
Timing evening meals at least three hours before bedtime allows adequate digestion. Research confirms that shorter dinner-to-bed intervals significantly increase GERD risk.
Avoiding trigger foods matters too. Fatty meals, spicy dishes, caffeine, and alcohol all increase reflux likelihood. Large portion sizes compound the problem by requiring longer digestion times.
Elevating the head of the bed by six to eight inches creates a gravity advantage. This isn’t the same as using multiple pillows, which can create uncomfortable bending. Bed risers or wedge-shaped supports work better.
Medical Interventions
For GERD-related nighttime symptoms, proton pump inhibitors effectively reduce acid production. Research indicates that bedtime H2-blockers may improve nocturnal gastric acid control in GERD patients.
Anti-nausea medications including ondansetron or promethazine can provide relief when other measures fail. These work through different mechanisms and suit different situations.
Treatment of underlying conditions—whether ulcers, gastroparesis, or other diagnoses—addresses the root cause rather than just symptoms.
When to Seek Medical Attention
Occasional nighttime nausea rarely signals serious problems. But certain patterns warrant medical evaluation.
See a doctor if:
- Nighttime vomiting occurs repeatedly over days or weeks
- Vomit contains blood or resembles coffee grounds
- Severe abdominal pain accompanies nausea
- Unexplained weight loss occurs alongside nocturnal symptoms
- Difficulty swallowing develops
- Symptoms persist despite basic lifestyle modifications
- New medications correlate with symptom onset
For individuals with neurological conditions or swallowing difficulties, any increase in nighttime symptoms deserves prompt evaluation. These populations face genuinely elevated aspiration risks.
Emergency warning signs include respiratory distress, chest pain, or signs of aspiration like coughing, choking, or breathing difficulties during or after vomiting episodes.
Common Myths About Vomiting During Sleep
Several misconceptions about sleep and vomiting persist despite medical evidence to the contrary.
Myth: People Regularly Vomit Without Waking
Community discussions often feature concerns about “silent aspiration” during sleep. While microaspiration of reflux can occur in GERD patients, actual vomiting without any arousal is extremely rare in neurologically intact individuals.
The protective reflexes described earlier make true unconscious vomiting unlikely. Most people who report waking up in vomit experienced partial arousal they don’t consciously remember.
Myth: Sleeping Position Doesn’t Matter
Position significantly affects reflux and nausea. Left-side sleeping reduces acid reflux for many people due to stomach anatomy. The gastroesophageal junction sits higher when lying on the left side, making reflux mechanically more difficult.
Back sleeping often worsens symptoms, while stomach sleeping presents mixed results—it may reduce reflux but can increase pressure on the abdomen.
Myth: Vomiting in Sleep Is Common After Drinking
While alcohol increases both nausea and reflux, most people wake before vomiting even when intoxicated. The danger lies in heavy intoxication that impairs protective reflexes and consciousness sufficiently to prevent normal awakening.
This is why alcohol poisoning carries serious aspiration risk—not because vomiting during sleep is normal, but because protective mechanisms become dangerously compromised.
Managing Specific Conditions That Cause Nighttime Nausea
GERD and Acid Reflux
Gastroesophageal reflux disease requires multi-pronged management. Acid suppression with PPIs or H2-blockers forms the pharmaceutical foundation. Lifestyle modifications including elevated sleeping position, dietary changes, and meal timing provide additional benefit.
Some patients require more aggressive interventions if standard treatment fails. Surgical options like fundoplication exist for severe, refractory cases.
Peptic Ulcer Disease
Ulcer treatment focuses on healing the damaged tissue and addressing underlying causes. Helicobacter pylori infection requires antibiotic therapy. NSAID-induced ulcers necessitate stopping the offending medication when possible.
Acid suppression allows healing, and avoiding long fasting periods reduces symptom intensity. Some people benefit from a light bedtime snack to buffer overnight acid production.
Gastroparesis
Delayed gastric emptying requires dietary modifications as a primary treatment. Small, frequent meals rather than large ones reduce stomach distension. Low-fat, low-fiber diets digest more easily.
Prokinetic medications that enhance gastric motility help some patients. Severe cases may require feeding tubes or gastric electrical stimulation.
Pregnancy-Related Nausea
Morning sickness management emphasizes safe, non-pharmaceutical approaches first. Eating small amounts frequently, keeping crackers at bedside, and avoiding empty stomach periods all help.
Ginger and vitamin B6 provide relief for many pregnant women. When symptoms become severe, prescription anti-nausea medications offer safe options for pregnancy.
Cyclic Vomiting Syndrome
This condition causes episodic, severe vomiting attacks that can occur at any time, including during sleep. The episodes often follow a predictable pattern for individual patients.
Management includes identifying and avoiding triggers, prophylactic medications to prevent episodes, and abortive treatments when episodes begin. Maintaining consistent sleep schedules helps some patients reduce episode frequency.
Frequently Asked Questions
It’s extremely unlikely for healthy individuals with normal neurological function to vomit while completely asleep. Protective airway reflexes automatically trigger awakening when stomach contents approach the throat. Most cases of “vomiting in sleep” involve partial arousal that the person doesn’t consciously remember. The body’s defense mechanisms work remarkably well to prevent aspiration in people with intact reflexes.
Several conditions cause middle-of-the-night vomiting including GERD, peptic ulcers, gastroparesis, low blood sugar, pregnancy-related nausea, and medication side effects. The horizontal sleeping position eliminates gravity’s help with keeping stomach contents down. Extended overnight fasting can trigger symptoms in conditions like ulcers or hypoglycemia. Acid reflux events commonly peak one to three hours after lying down when reflux is most likely to occur.
Sleep with the head elevated by six to eight inches using bed risers or a wedge pillow. Position on the left side, which reduces reflux due to stomach anatomy. Keep a basin nearby and sit up completely if nausea intensifies. Avoid eating within three hours of bedtime to reduce stomach contents. For high-risk individuals with neurological conditions, medical positioning devices and monitoring may be necessary to ensure safety during sleep.
Seek immediate medical attention if vomiting is accompanied by severe abdominal pain, chest pain, difficulty breathing, blood in vomit, signs of dehydration, altered mental status, or if aspiration is suspected based on coughing, choking, or respiratory distress. Repeated vomiting that prevents keeping down liquids for more than 12 hours, particularly in vulnerable populations like children or elderly individuals, also warrants prompt evaluation to prevent complications.
Yes, sleeping position significantly impacts both reflux and aspiration risk. Left-side sleeping reduces acid reflux because the gastroesophageal junction sits higher due to stomach anatomy. Elevated head positioning creates a gravity advantage that reduces reflux episodes. Back sleeping often worsens reflux symptoms. For individuals with impaired consciousness or swallowing difficulties, side-lying positions allow fluids to drain from the mouth rather than pooling in the throat where aspiration risk increases.
Individuals with severe GERD, gastroparesis, cyclic vomiting syndrome, or persistent nausea from any cause experience more frequent nighttime vomiting episodes. However, protective reflexes still typically trigger awakening before vomiting occurs. People with neurological impairments affecting brainstem function, stroke survivors with swallowing difficulties, those with altered consciousness from medication or medical conditions, and individuals with learning disabilities affecting swallowing mechanics face genuinely elevated risks because their protective reflexes may be compromised.
Yes, anxiety significantly affects digestive function and can cause nighttime nausea. Stress influences gut motility, acid production, and visceral sensitivity. Some people experience anticipatory anxiety about the coming day that manifests as early morning or nighttime stomach upset. The gut-brain connection runs deep, and psychological factors produce very real physical symptoms. Treating underlying anxiety disorders often reduces associated digestive symptoms including nocturnal nausea and vomiting episodes.
Conclusion: Understanding Your Body’s Protective Mechanisms
The human body evolved remarkable defenses against aspiration, and these protective reflexes remain active throughout sleep. For healthy individuals with intact neurological function, vomiting while completely unconscious is extraordinarily rare.
That said, nighttime nausea and vomiting that wake people from sleep are common experiences with multiple potential causes. GERD, peptic ulcers, gastroparesis, low blood sugar, pregnancy, medications, and anxiety all contribute to nocturnal symptoms.
Understanding when nighttime vomiting represents a normal response to illness versus a potentially serious condition helps determine appropriate action. Occasional episodes related to obvious causes like viral gastroenteritis rarely warrant concern. Recurrent nighttime vomiting, particularly with warning signs like blood, severe pain, or weight loss, requires medical evaluation.
For those concerned about aspiration risk—whether for themselves or someone they’re caring for—remember that risk stratifies dramatically based on neurological status and protective reflex function. Healthy individuals can rest assured their bodies will wake them if needed. Those with compromised reflexes benefit from preventive positioning and medical guidance.
If nighttime nausea or vomiting disrupts sleep repeatedly, don’t dismiss it as something to simply endure. Effective treatments exist for most underlying causes, and proper diagnosis leads to targeted management that can restore restful sleep and reduce symptoms significantly. Schedule an evaluation with a gastroenterologist or primary care provider to identify the cause and develop an appropriate treatment plan.