
Quick Summary: Yes, living with one lung is medically possible. Research published on PubMed shows that after pneumonectomy (lung removal surgery), most patients experience approximately 30-36% reduction in lung function but can still perform daily activities without supplemental oxygen. The remaining lung adapts over time, though physical limitations and reduced exercise capacity are common.
The human respiratory system seems designed with redundancy in mind. While most people have two lungs working together to oxygenate blood and remove carbon dioxide, a surprising number of individuals live full lives with just one functioning lung.
But how does the body manage this dramatic change? What happens when half the respiratory capacity disappears overnight?
The reality is more nuanced than simple mathematics would suggest. Losing one lung doesn’t mean losing exactly 50% of respiratory function, and survival isn’t just possible—many patients return to relatively normal activities.
Why Would Someone Need a Lung Removed?
Pneumonectomy, the surgical removal of an entire lung, isn’t a common procedure. Doctors reserve this operation for serious medical conditions where no other treatment option exists.
Lung cancer represents the most frequent reason for pneumonectomy. When tumors grow too large or spread throughout one lung, complete removal becomes necessary to prevent further metastasis.
Other conditions requiring lung removal include severe tuberculosis, traumatic injury that destroys lung tissue beyond repair, and certain congenital abnormalities. Chronic infections that don’t respond to medication sometimes necessitate this drastic intervention.
According to research published in the Journal of the American College of Surgeons, pneumonectomies comprised 10.8% of non-small cell lung cancer resections in 1988 but only 2.9% by 2010. This dramatic decline reflects improved surgical techniques that allow surgeons to remove smaller portions—individual lobes rather than entire lungs—in most cases.
How the Body Adapts to Single Lung Function
Here’s where things get interesting. The human body demonstrates remarkable compensatory abilities when faced with reduced lung capacity.
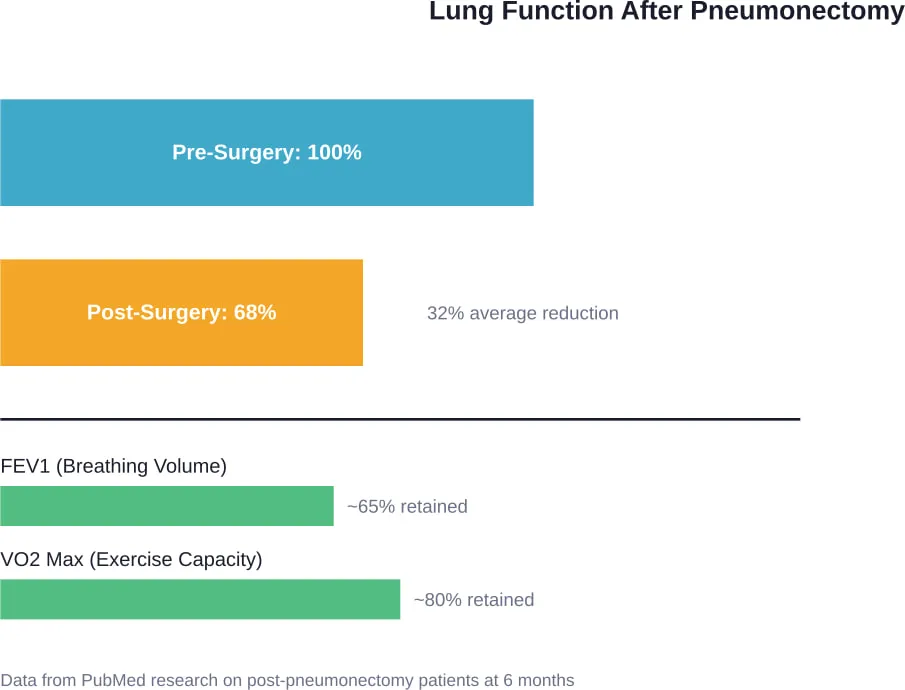
Research findings published on PubMed indicate that despite worsening of lung function by approximately 32-36% after pneumonectomy, most patients adjust to living with only one lung. The key word here is “approximately 30%”—not the expected 50%.
So what explains this discrepancy?
The remaining lung doesn’t just sit idle. It undergoes structural and functional changes to partially compensate for the missing organ. Blood vessels redistribute flow, the heart adjusts its pumping patterns, and breathing mechanics shift to maximize oxygen uptake.
One study following patients six months post-pneumonectomy found an average decrease of 32-36% in FEV1 (forced expiratory volume), FVC (forced vital capacity), and DLCO (diffusing capacity), with approximately 20% reduction in VO2 max. These numbers represent substantial decreases, certainly, but they’re far from the 50% loss that simple arithmetic would predict.
Physical Limitations and Daily Life
Living with one lung doesn’t mean returning to pre-surgery capabilities without any changes. Physical limitations exist, though they vary considerably between individuals.
Most pneumonectomy patients don’t require supplemental oxygen for daily activities. That’s a critical distinction—the remaining lung typically provides adequate oxygenation for rest and moderate activity.
Exercise capacity, however, takes a noticeable hit. The 20% reduction in VO2 max means strenuous physical activities become more challenging. Running, climbing stairs, and carrying heavy objects require more effort and frequent rest breaks.
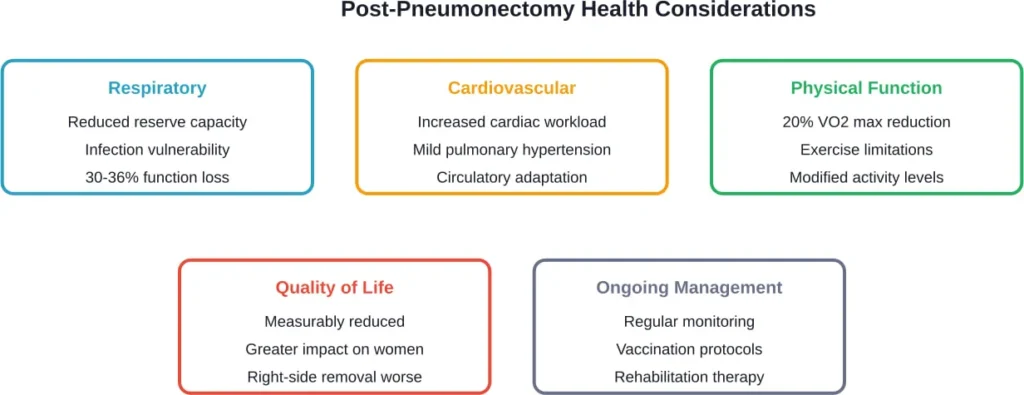
Research indicates quality of life after pneumonectomy is significantly lower compared to age- and gender-matched populations, especially in women after right-sided pneumonectomy. The right lung is typically larger and contributes more to overall respiratory function, making its loss more impactful.
What Activities Remain Possible?
Despite reduced capacity, many patients return to work and resume hobbies. Sedentary and light-activity occupations pose few problems. Walking, light household chores, and social activities generally remain manageable.
The body learns its new limits through gradual rehabilitation. Physical therapy helps patients understand their revised capabilities and develop strategies to conserve energy during daily tasks.
Community discussions among pneumonectomy patients reveal that adaptation is highly individual. Some people report minimal lifestyle changes, while others describe significant ongoing limitations.
Medical Complications and Long-Term Concerns
Pneumonectomy carries both immediate surgical risks and long-term health considerations. Understanding these helps set realistic expectations.
Pulmonary hypertension represents one potential complication. With only one lung processing all blood flow, pressure in pulmonary blood vessels can increase. Research published on PubMed indicates this complication is uncommon and, when present, usually only mild to moderate.
Cardiovascular stress increases as the heart works harder to maintain adequate oxygen delivery. The remaining lung must handle 100% of gas exchange responsibilities, which can strain the system during illness or exertion.
Respiratory infections pose heightened risks. With reduced lung capacity, pneumonia or bronchitis can quickly become serious. Vaccinations and prompt treatment of respiratory symptoms become essential preventive measures.
Age and Surgical Outcomes
Patient age significantly influences both short-term and long-term outcomes after pneumonectomy. Research published in the Journal of the American College of Surgeons examined survival rates across different age groups.
Short-term outcomes of morbidity, mortality, and quality of life worsen with increasing age. Elderly patients face higher surgical risks and longer recovery periods.
The study stratified ages as under 50, 50-69, 70-79, and 80 or older, comparing pneumonectomy patients’ overall survival to matched patients who refused surgery and underwent radiation therapy instead. Results showed that younger patients tolerated the procedure better and achieved better functional outcomes.
This doesn’t mean elderly patients can’t survive pneumonectomy, but it does highlight the importance of careful patient selection and realistic expectation-setting before surgery.
Frequently Asked Questions
Lifespan depends primarily on the underlying condition that necessitated lung removal. For cancer patients, five-year survival rates vary based on cancer stage and type. For those who had pneumonectomy due to trauma or infection, lifespan can approach normal if the remaining lung stays healthy. Overall health, age at surgery, and ongoing medical management all influence longevity.
Most pneumonectomy patients don’t require supplemental oxygen for daily activities. The remaining lung typically provides adequate oxygenation at rest and during moderate activity. However, oxygen may be needed during illness, at high altitudes, or in some cases during strenuous exercise. Individual circumstances vary considerably.
Human lungs don’t regenerate lost tissue or grow new lobes. However, the remaining lung does undergo compensatory changes—blood vessels redistribute, breathing mechanics adjust, and efficiency improves somewhat over time. This adaptation explains why functional loss is less than 50%, but it’s compensation rather than true regeneration.
Pneumonectomy removes an entire lung, while lobectomy removes only one lobe (section) of a lung. Each lung has multiple lobes—three on the right, two on the left. Lobectomy is far more common and causes less functional impairment. Surgeons perform lobectomy whenever possible, reserving pneumonectomy for cases where disease affects the entire lung.
Initial hospital stays typically last 7-14 days barring complications. Full recovery extends much longer—generally 6-12 months before patients reach their new functional baseline. Physical therapy and pulmonary rehabilitation continue throughout this period. The first few months involve the most dramatic improvements as the body adapts.
Generally speaking, activities requiring sustained high oxygen demand become problematic. Competitive sports, heavy lifting, running long distances, and working at high altitudes may exceed capacity. Scuba diving is typically prohibited due to pressure-related risks. Individual tolerance varies, and rehabilitation specialists help determine personal safe activity levels.
Yes. Research shows right-sided pneumonectomy typically causes greater functional impairment than left-sided removal. The right lung is larger and has three lobes compared to the left lung’s two lobes. Studies indicate quality of life decreases more significantly after right pneumonectomy, particularly in women.
Conclusion
Living with one lung is medically possible and, for many patients, compatible with reasonable quality of life. The body’s compensatory mechanisms prevent the catastrophic 50% function loss that simple math would predict.
That said, pneumonectomy isn’t without significant impact. Reduced exercise capacity, heightened infection risks, and measurably lower quality of life represent real challenges that patients face long-term.
For those facing this surgery, understanding both the possibilities and limitations helps set realistic expectations. Medical advances continue improving outcomes, and rehabilitation protocols help patients maximize their remaining respiratory capacity.
If pneumonectomy is recommended for you or someone you care about, discuss specific prognosis factors with thoracic surgeons and pulmonologists who can provide personalized guidance based on individual health status and circumstances.