
Quick Summary: Gestational diabetes causes high blood sugar during pregnancy, typically developing in the second or third trimester and usually resolving after birth. According to the CDC, about 8% of women who had a live birth developed gestational diabetes in 2021, and it increases risks for both mother and baby, including larger birth weight, preeclampsia, and future type 2 diabetes. With proper management through diet, exercise, and sometimes medication, most women deliver healthy babies and see their blood sugar return to normal post-delivery.
Getting a gestational diabetes diagnosis can feel overwhelming. One moment you’re sailing through pregnancy, the next you’re facing a condition that sounds serious and complicated.
But here’s the thing—gestational diabetes is manageable. According to the CDC, about 8% of women who had a live birth developed gestational diabetes in 2021. You’re definitely not alone in this.
This guide breaks down exactly what happens when you have gestational diabetes, from immediate pregnancy effects to long-term health considerations. No medical jargon, just the facts.
Understanding What Gestational Diabetes Actually Does
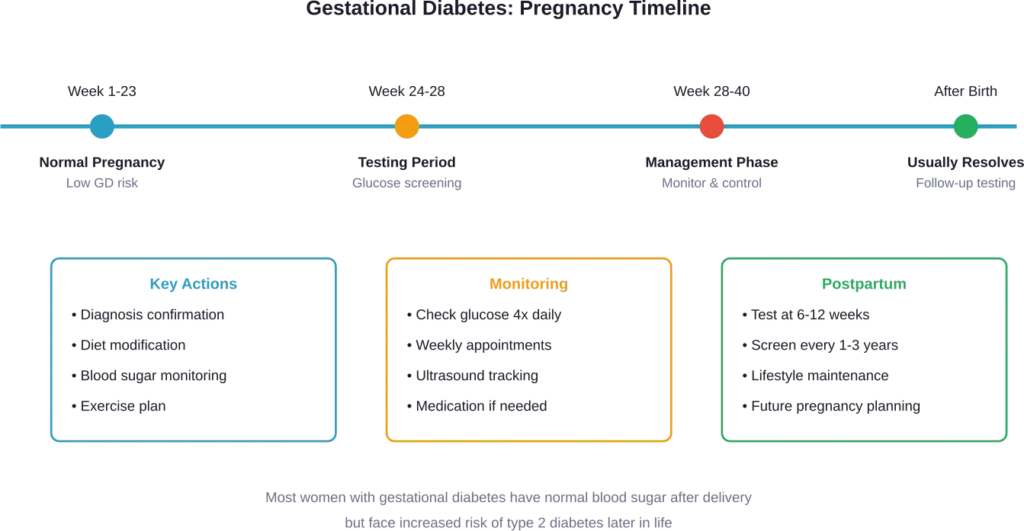
Gestational diabetes is high blood sugar that develops during pregnancy. The condition typically appears between the 24th and 28th week of pregnancy, though it can develop earlier.
The root cause? Hormonal changes during pregnancy affect how the body processes insulin. The placenta produces hormones that help the baby develop, but these same hormones make cells more resistant to insulin. When the body can’t produce enough extra insulin to overcome this resistance, blood glucose levels rise.
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) explains that gestational diabetes means the body can’t make the extra insulin needed during pregnancy. This isn’t anyone’s fault—it’s a biological response to pregnancy hormones.
Why Blood Sugar Levels Matter
Glucose crosses the placenta and provides energy for the baby’s growth. But too much glucose creates problems. When blood sugar remains elevated, the baby receives more glucose than needed, which triggers their pancreas to produce extra insulin.
This excess insulin acts as a growth hormone. The result? A larger-than-average baby, which doctors call macrosomia.
What Happens During Your Pregnancy
Most women with gestational diabetes have otherwise normal pregnancies. That’s important to understand right from the start. The condition is manageable, and with proper care, serious complications are preventable.
That said, unmanaged gestational diabetes increases certain pregnancy risks.
Effects on the Baby
The most common concern is excessive birth weight. Babies born to mothers with gestational diabetes often weigh more than 9 pounds. This can lead to:
- More difficult vaginal delivery
- Higher likelihood of cesarean delivery
- Shoulder injuries during birth (shoulder dystocia)
- Low blood sugar immediately after birth (neonatal hypoglycemia)
- Breathing difficulties
- Jaundice
According to research published through the National Institutes of Health, about 85 to 90% of all diabetes in pregnancy is gestational diabetes, and most women with gestational diabetes have otherwise normal pregnancies.
Real talk: these risks sound scary, but they’re significantly reduced with proper monitoring and blood sugar control.
Effects on the Mother
Women with gestational diabetes face increased risk for certain pregnancy complications. The NIDDK notes that the risk of preeclampsia—dangerously high blood pressure during pregnancy—doubles compared to women without gestational diabetes.
Other maternal risks include:
- Preeclampsia (high blood pressure and organ stress)
- Increased chance of cesarean delivery
- Polyhydramnios (excess amniotic fluid)
- Premature birth
According to CDC data analyzing pregnancies in Massachusetts from 1998-2007, women with gestational diabetes during any pregnancy showed increased prevalence of adverse birth outcomes compared to women without diabetes.
How Gestational Diabetes Gets Managed
Management focuses on controlling blood sugar levels. For most women, this doesn’t mean dramatic lifestyle overhauls—it means making strategic adjustments.
Diet Modifications
Nutrition becomes the primary tool for blood sugar control. A healthcare team typically includes a registered dietitian who creates an eating plan tailored to individual needs.
The goal isn’t restriction—it’s balance. Carbohydrates affect blood sugar most directly, so managing carb intake throughout the day helps keep glucose levels steady.
Physical Activity
Exercise helps cells use glucose more effectively, which lowers blood sugar naturally. The American College of Obstetricians and Gynecologists (ACOG) recommends 30 minutes of moderate-intensity aerobic exercise at least 5 days per week—or a minimum of 150 minutes weekly.
Walking is the most commonly recommended activity. It’s safe, effective, and doesn’t require special equipment.
Blood Sugar Monitoring
Frequent testing becomes part of daily routine. Most women check their blood sugar four times daily: once in the morning before eating (fasting) and again after each meal.
This isn’t just busywork. These numbers tell the healthcare team whether current management strategies are working or need adjustment.
Medication When Needed
Some women with gestational diabetes may need diabetes medicine to manage blood glucose levels. This doesn’t mean the condition is worse or that management has failed. Some bodies simply need extra help during pregnancy.
Insulin is the most common treatment. It doesn’t cross the placenta, so it doesn’t affect the baby directly. Some doctors prescribe metformin, an oral medication, though insulin remains the gold standard.
| Management Strategy | Typical Implementation | Success Rate |
|---|---|---|
| Diet modification | Carb counting, balanced meals, portion control | Many women can manage blood glucose levels by following a healthy eating plan |
| Exercise | 30 min/day, 5 days/week moderate activity | Enhances diet effectiveness |
| Blood sugar monitoring | 4 times daily (fasting + post-meals) | Essential for all cases |
| Insulin therapy | Injections 1-4 times daily as prescribed | Insulin is usually the first choice of diabetes medicine for gestational diabetes |
| Oral medication | Metformin tablets, usually twice daily | May be effective |
What Happens After Delivery
Here’s some good news: gestational diabetes usually disappears after the baby is born. In most cases, blood sugar levels return to normal within hours or days of delivery.
But the story doesn’t end there.
Immediate Postpartum Period
Healthcare providers test blood sugar levels shortly after delivery to confirm they’ve normalized. If blood sugar remains elevated, it may indicate type 2 diabetes that was present before pregnancy but undiagnosed—not true gestational diabetes.
The baby also needs monitoring. Newborns whose mothers had gestational diabetes face higher risk for low blood sugar (hypoglycemia) in the first hours after birth. Hospital staff check the baby’s glucose levels and watch for signs of breathing difficulties.
Long-Term Health Implications
This is where things get serious. Women who’ve had gestational diabetes face significantly increased risk of developing type 2 diabetes later in life.
According to CDC research analyzing birth data, women with gestational diabetes or other diabetes during pregnancy have increased risk for type 2 diabetes. Research found that women with very preterm births (2%) had an increased type 2 diabetes risk (adjusted hazard ratio 1.34; 95% confidence interval [CI], 1.05–1.71), with this increased risk emerging in the decade following pregnancy.
The exact percentage varies across studies, but the message is consistent: gestational diabetes serves as a warning sign for future metabolic health.
Reducing Future Diabetes Risk
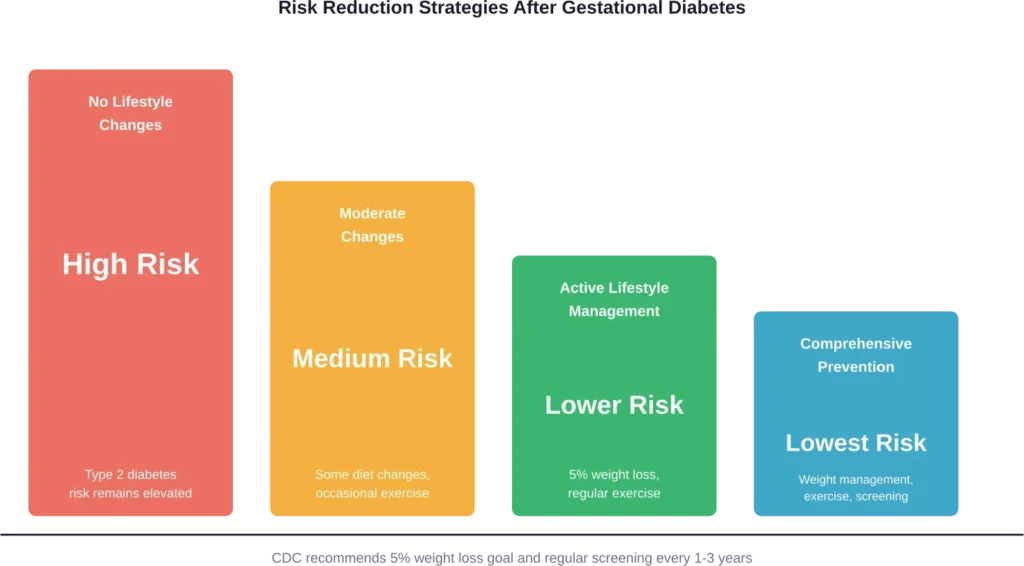
The CDC provides specific guidance for reducing type 2 diabetes risk after gestational diabetes. Their recommendations include:
- Setting a weight loss goal of 5% of starting weight if overweight
- Allowing time for postpartum recovery before aggressive weight loss
- Maintaining regular physical activity
- Getting tested for diabetes 6-12 weeks after delivery
- Continuing diabetes screening every 1-3 years
That 5% weight loss target is evidence-based. Research shows that modest weight reduction significantly decreases diabetes risk in women with previous gestational diabetes.
Impact on Future Pregnancies
Women who’ve had gestational diabetes in one pregnancy are more likely to develop it again in subsequent pregnancies. Planning future pregnancies with healthcare provider input helps optimize health before conception.
Some women do develop type 2 diabetes between pregnancies. Preconception testing ensures any existing diabetes gets identified and managed before the next pregnancy begins.
Effects on Children’s Long-Term Health
Babies born to mothers with gestational diabetes face their own long-term considerations. Research published in medical journals indicates that in utero exposure to gestational diabetes is associated with increased risk of childhood obesity and metabolic issues.
The mechanism involves fetal programming. High glucose exposure during critical developmental periods may alter how the child’s metabolism functions throughout life.
This doesn’t mean these outcomes are inevitable. Breastfeeding, healthy childhood nutrition, and active lifestyles all help mitigate these risks.
Managing the Emotional Impact
Getting diagnosed with any medical condition during pregnancy triggers anxiety. That’s completely normal.
Many women report feeling guilt, as though they caused the condition. Let’s be clear: gestational diabetes isn’t caused by eating too much sugar or not exercising enough. It’s a physiological response to pregnancy hormones combined with genetic and environmental factors.
The diagnosis doesn’t reflect personal failure. It’s simply information about how the body is responding to pregnancy.
According to qualitative research analyzing mothers’ perceptions, many women express uncertainty about long-term outcomes for their children after gestational diabetes exposure. Healthcare providers can help by providing clear information about risks and actionable prevention strategies.
Special Considerations and Risk Factors
Certain factors increase the likelihood of developing gestational diabetes:
- Being overweight or obese before pregnancy
- Having a family history of type 2 diabetes
- Previously delivering a baby weighing over 9 pounds
- Having had gestational diabetes in a prior pregnancy
- Having polycystic ovary syndrome (PCOS)
- Being older than 25
- Certain racial and ethnic backgrounds (higher rates in Hispanic, Black, Native American, and Asian women)
These risk factors don’t guarantee gestational diabetes will develop. They simply indicate increased probability, which is why screening happens for all pregnant women.
| Risk Factor | Impact on GD Risk |
|---|---|
| Previous gestational diabetes | High—increases likelihood in future pregnancies |
| BMI over 30 | Moderate to high increase |
| First-degree relative with diabetes | Moderate increase |
| Age over 35 | Moderate increase |
| PCOS | Moderate increase |
| Previous baby over 9 lbs | Moderate increase |
When Medical Intervention Becomes Critical
Most cases of gestational diabetes are managed successfully with monitoring and lifestyle adjustments. But some situations require more intensive medical intervention.
Signs that warrant immediate contact with healthcare providers include:
- Blood sugar readings consistently above target ranges
- Symptoms of very high blood sugar (extreme thirst, frequent urination, blurred vision, fatigue)
- Decreased fetal movement
- Signs of preeclampsia (severe headache, vision changes, upper abdominal pain, sudden swelling)
These situations are uncommon when gestational diabetes is properly managed, but recognizing warning signs ensures prompt treatment if complications arise.
Frequently Asked Questions
Most women’s blood sugar returns to normal after delivery. However, you should get tested 6-12 weeks postpartum to confirm. According to the CDC, women with gestational diabetes face increased risk of developing type 2 diabetes later in life, which is why ongoing screening every 1-3 years is recommended.
Yes, many women with gestational diabetes deliver vaginally. However, if the baby grows very large (macrosomia), doctors may recommend cesarean delivery to reduce risks of birth complications like shoulder dystocia. Your healthcare team will monitor baby’s size through ultrasounds and discuss delivery options.
Absolutely not. Gestational diabetes results from how pregnancy hormones affect insulin function, combined with genetic predisposition and other factors beyond your control. The NIDDK emphasizes that it occurs when the body can’t make enough extra insulin needed during pregnancy—it’s not caused by eating sugar or lack of willpower.
Most women check blood sugar four times daily: once in the morning before eating (fasting) and one to two hours after each meal. Your healthcare provider will give you specific target ranges and instructions. Frequent monitoring provides the data needed to adjust your management plan and ensure both you and baby stay healthy.
Yes, breastfeeding is safe and encouraged after gestational diabetes. In fact, breastfeeding may help reduce your long-term risk of developing type 2 diabetes. It also provides health benefits for your baby, potentially reducing their future obesity and diabetes risk.
Many women manage gestational diabetes through diet and exercise alone. The remaining women need medication—usually insulin—to keep blood sugar controlled. If lifestyle changes aren’t sufficient after a trial period (typically 1-2 weeks), your provider will discuss medication options. This isn’t a failure; some bodies simply need pharmaceutical support during pregnancy.
There’s no absolute forbidden foods list, but managing carbohydrate intake is key. Foods that spike blood sugar quickly—sugary drinks, white bread, pastries, candy—should be limited. Your dietitian will help you understand portion sizes and timing. The focus is on balanced meals with protein, healthy fats, fiber-rich carbohydrates, and vegetables rather than strict elimination.
Moving Forward With Confidence
Gestational diabetes changes your pregnancy experience, but it doesn’t have to derail it. With appropriate management, the vast majority of women deliver healthy babies and see their blood sugar normalize after birth.
The diagnosis does serve as an important health signal. It indicates increased risk for type 2 diabetes in the future, which makes post-pregnancy lifestyle choices particularly important. That 5% weight loss goal the CDC recommends? It’s achievable and makes a real difference.
Work closely with your healthcare team. Check your blood sugar as directed. Follow the eating plan. Stay active within safe limits. These steps protect both you and your baby.
And remember—you’re managing this condition successfully every time you check your blood sugar, choose a balanced meal, or take a walk. That’s not just getting through pregnancy. That’s taking control of long-term health.
If you’ve been recently diagnosed, talk to your healthcare provider about creating a management plan tailored to your specific situation. The sooner you start active management, the better the outcomes for everyone involved.