Quick Summary: Receiving the wrong blood type can trigger a hemolytic transfusion reaction, where the immune system attacks incompatible red blood cells, potentially causing fever, kidney failure, shock, or death. According to the National Institutes of Health, acute reactions occur within 24 hours and can be life-threatening, though proper blood typing and cross-matching prevent most cases.
Blood transfusions save millions of lives each year. But when incompatible blood enters your system, the consequences can be catastrophic.
The human immune system is designed to protect against foreign invaders. When the wrong blood type is transfused, your body recognizes the unfamiliar blood cells as threats and launches an immediate attack. This process, called a hemolytic transfusion reaction, can escalate from mild symptoms to life-threatening complications within minutes.
Here’s what actually happens when blood types don’t match.
Understanding Blood Type Compatibility
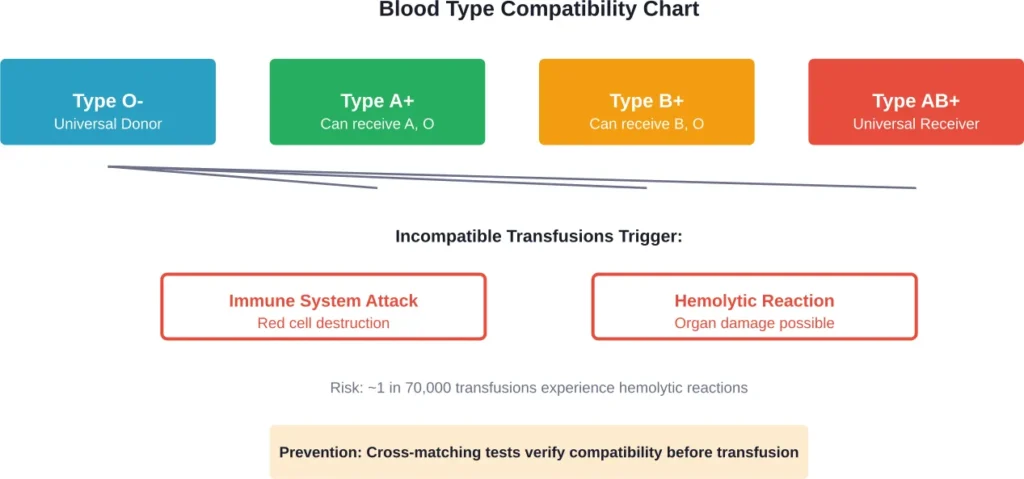
Human blood is classified by the presence or absence of specific antigens on red blood cell surfaces. These antigens—primarily A, B, and Rh factor—determine your blood type (A, B, AB, or O, each positive or negative).
Your plasma naturally contains antibodies against antigens you don’t possess. Someone with type A blood has anti-B antibodies. Type B blood contains anti-A antibodies. Type O blood contains both anti-A and anti-B antibodies, while type AB blood has neither.
This is where compatibility becomes critical.
When someone with type A blood receives type B blood, their anti-B antibodies immediately recognize the B antigens as foreign. The immune response begins within seconds.
The Hemolytic Transfusion Reaction
According to the National Institutes of Health, hemolytic transfusion reactions occur at a rate of approximately 1 in 70,000 units transfused. These reactions are classified as acute (within 24 hours) or delayed (days to weeks later).
Acute hemolytic reactions are the most dangerous.
The moment incompatible blood enters circulation, antibodies bind to the foreign red blood cells and mark them for destruction. This process—called hemolysis—causes the cells to rupture and release their contents into the bloodstream.
What Happens in Your Body
The destruction of red blood cells releases hemoglobin directly into plasma. Free hemoglobin is toxic to kidneys and can cause acute renal failure. The cell fragments trigger widespread inflammation and activate the blood clotting cascade.
Patients often experience the first symptoms during the transfusion itself. Fever and chills are typically the earliest signs, followed by back pain, chest tightness, and difficulty breathing. Red or dark brown urine indicates hemoglobinuria—free hemoglobin being filtered through the kidneys.
But it gets worse.
As the reaction progresses, blood pressure drops dangerously low. The massive release of inflammatory molecules can trigger shock and disseminated intravascular coagulation (DIC), where blood clots form throughout small vessels while bleeding occurs elsewhere. Organ damage accumulates rapidly.
Symptoms and Severity
| Symptom Category | Early Signs | Severe Complications |
|---|---|---|
| General | Fever, chills, anxiety | Shock, loss of consciousness |
| Cardiovascular | Rapid heartbeat, chest pain | Hypotension, cardiac arrest |
| Respiratory | Shortness of breath | Acute respiratory distress |
| Renal | Dark urine, reduced output | Acute kidney failure |
| Hematologic | Back pain, hemoglobinuria | DIC, severe bleeding |
The severity depends on the volume of incompatible blood transfused and how quickly the reaction is recognized. Even small amounts—as little as 10-15 milliliters—can trigger symptoms in highly incompatible transfusions.
StatPearls research notes that immune-mediated hemolytic transfusion reactions result from mismatch or incompatibility between patient and donor products. Non-immune reactions can also occur from mechanical damage to red cells or improper storage, though these are less severe.
Delayed Hemolytic Reactions
Not all reactions happen immediately.
Delayed hemolytic transfusion reactions occur after 24 hours, typically presenting around 2 weeks after transfusion in previously transfused or pregnant patients. These individuals may have developed antibodies to minor blood group antigens that aren’t detected in standard screening because antibody levels have declined over time.
When exposed again to the same antigen, the immune system mounts an anemnestic response—antibody levels surge rapidly, destroying the transfused cells. In sickle cell disease patients, delayed hemolytic transfusion reactions can be particularly severe and may progress to complications including hyperhemolysis.
Prevention and Safety Measures
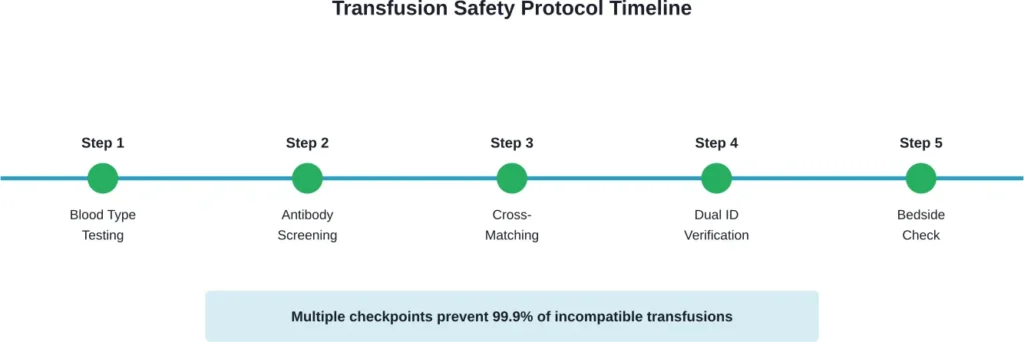
Modern blood banking has implemented multiple safety barriers to prevent wrong blood type transfusions:
- Blood typing determines ABO and Rh status
- Antibody screening detects unexpected antibodies
- Cross-matching mixes patient serum with donor cells to verify compatibility
- Two-person verification confirms patient identity and blood unit match
- Bedside checks before transfusion begins
The World Health Organization emphasizes that all activities related to blood collection, testing, processing, storage, and distribution should be coordinated nationally through effective organization and quality management systems.
Despite these protocols, human error remains the leading cause of transfusion reactions. Mislabeling samples, failing to verify patient identity, or administering blood to the wrong patient can bypass technical safeguards.
Treatment and Prognosis
When a hemolytic transfusion reaction is suspected, the transfusion must stop immediately. Every minute matters.
Treatment focuses on maintaining blood pressure, protecting kidney function, and managing complications. Intravenous fluids help flush hemoglobin through the kidneys. Medications support blood pressure and urine output. Severe cases may require dialysis if kidney failure develops.
The prognosis depends on reaction severity and how quickly treatment begins. Mild reactions may resolve with supportive care. Severe reactions can result in permanent organ damage or death, particularly if large volumes of incompatible blood were transfused before the reaction was recognized.
Frequently Asked Questions
Yes, survival is possible if the reaction is caught early and the transfusion stopped immediately. Mild incompatibilities or small volumes may cause only minor symptoms. However, severe reactions involving major blood group incompatibility and large volumes can be fatal without prompt intervention.
Acute hemolytic reactions typically begin during the transfusion or within 24 hours. Symptoms can appear within minutes for severe ABO incompatibilities. Delayed reactions occur after 24 hours, typically presenting around 2 weeks after transfusion as antibody levels rise.
Fever and chills are usually the earliest symptoms, often accompanied by anxiety, back pain, chest discomfort, and difficulty breathing. Red or brown urine indicates severe hemolysis. Any unexplained symptoms during transfusion should prompt immediate evaluation.
Hemolytic transfusion reactions occur in approximately 1 in 70,000 transfused units, according to NIH data. Fatal reactions are even rarer due to modern safety protocols, though exact rates vary by healthcare system and reporting standards.
Type O negative blood is the universal donor because it lacks A, B, and Rh antigens. It can be given to patients of any blood type in emergencies when there’s no time for cross-matching, though type-specific blood is always preferred when available.
No medication can prevent hemolytic reactions caused by blood type incompatibility. The only prevention is proper blood typing, antibody screening, and cross-matching before transfusion. Some facilities give antihistamines or acetaminophen to reduce allergic or febrile reactions, but these don’t address immune hemolysis.
People with type O blood have both anti-A and anti-B antibodies, making them particularly vulnerable if they receive A, B, or AB blood. However, the reaction severity depends more on the volume transfused and the specific antibodies present than on the recipient’s blood type alone.
Conclusion
Receiving the wrong blood type triggers an immune cascade that can destroy red blood cells, damage organs, and threaten life within hours. The hemolytic transfusion reaction represents one of the most serious complications in modern medicine.
But here’s the thing—it’s also one of the most preventable.
Multiple safety barriers exist precisely because the consequences are so severe. Blood typing, cross-matching, and verification protocols have made fatal transfusion reactions exceedingly rare in developed healthcare systems. According to the World Health Organization, nearly 120 million blood units are donated globally each year, with proper testing and coordination preventing countless potential reactions.
If you’re scheduled for surgery or a procedure that might require transfusion, don’t hesitate to ask about blood safety protocols. Understanding your blood type and ensuring accurate identification throughout your care can provide additional peace of mind. The medical system has robust safeguards in place, but patient awareness adds another layer of protection against this rare but serious complication.