
Quick Summary: Skipping Pap smears significantly increases your risk of developing undetected cervical cancer, which can progress from early, highly treatable stages to advanced disease with a much lower survival rate. According to CDC data, when cervical cancer is diagnosed at an early stage, the five-year survival rate is 91%. The overall five-year relative survival rate for cervical cancer is 67.4%. Without screening, precancerous cell changes go unnoticed, and HPV infections that cause approximately 80% of cervical cancers in sexually active individuals remain undetected until potentially too late.
Cervical cancer screening has been called one of the most important public health achievements of the 20th century. Over the past 50 years, cervical cancer deaths in the United States have decreased more than 50%, thanks largely to regular Pap testing.
But here’s the concerning reality: around 13,000 women are diagnosed with cervical cancer annually in the United States, and approximately 4,000 die from it each year. Many of these cases occur in women who haven’t been screened according to recommended guidelines.
So what actually happens when someone never gets a Pap smear? The consequences extend far beyond a missed appointment.
The Silent Progression of Cervical Cancer
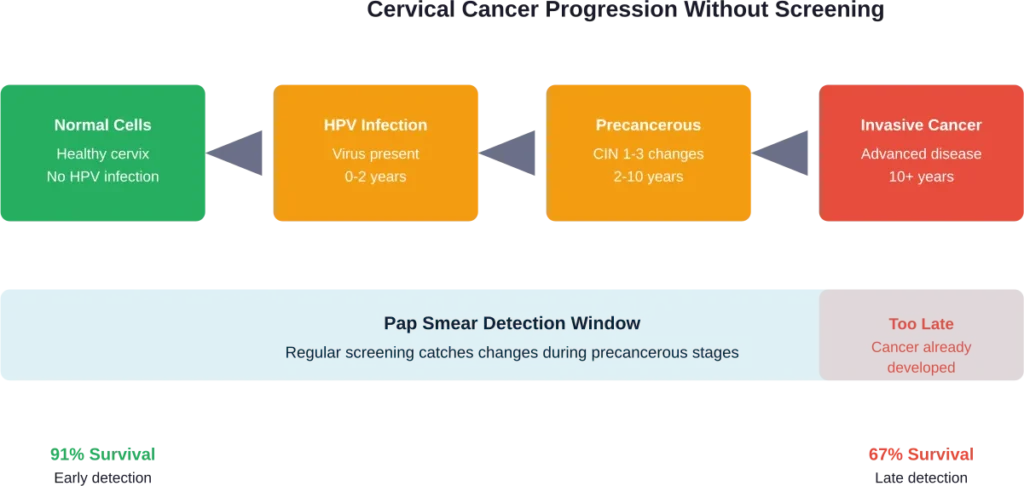
Cervical cancer doesn’t develop overnight. It’s a slow-moving disease that typically takes many years to progress from normal cells to precancerous changes to invasive cancer.
This gradual timeline is precisely why screening works so well—and why skipping it is so dangerous.
Human papillomavirus (HPV) is responsible for causing the vast majority of cervical cancer cases. The CDC notes that the HPV test looks for the virus that can cause cell changes on the cervix, while the Pap test looks for abnormal cells themselves.
Without screening, HPV infections persist undetected. Cell changes develop silently. Precancerous lesions advance without intervention.
The disease progresses through distinct stages, but without a Pap smear, there’s no early warning system.
From HPV Infection to Cancer
Research shows that approximately 80% of sexually active Americans have HPV at some point, and many don’t know it. Most HPV infections clear on their own within two years.
But some don’t.
Persistent high-risk HPV infections can cause cellular changes called cervical intraepithelial neoplasia (CIN). These precancerous changes are exactly what Pap smears detect—before they become cancer.
Skip the screening, and these changes go unnoticed. They progress from CIN 1 (mild dysplasia) to CIN 2 and CIN 3 (moderate to severe dysplasia), and eventually to invasive cervical cancer.
The Survival Rate Gap
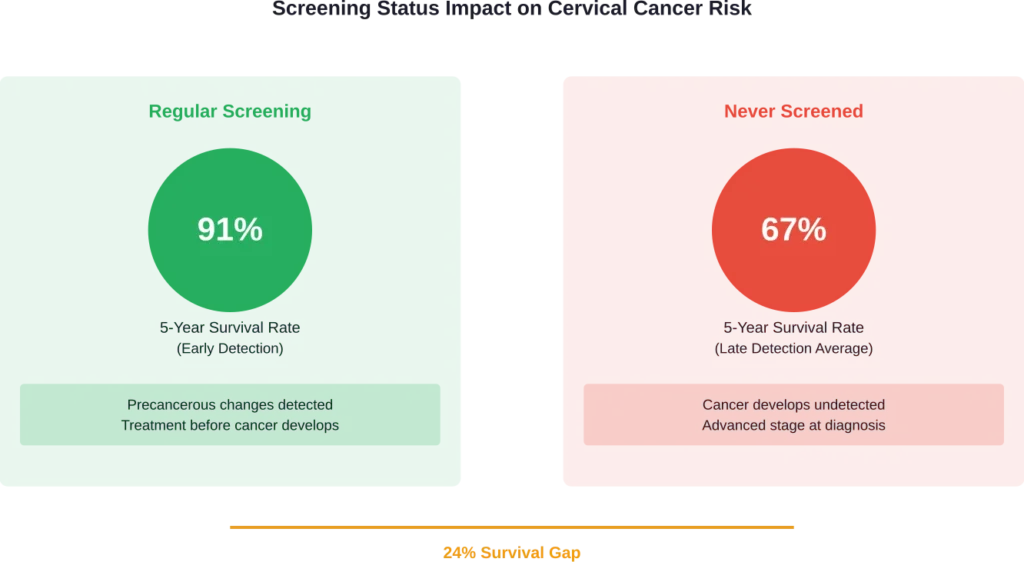
The difference between early detection and late detection is stark.
According to CDC data, when cervical cancer is diagnosed at an early stage, the five-year survival rate is 91%. But the overall five-year relative survival rate for cervical cancer is 67.4%. Why the gap?
Because many cases aren’t caught early. They’re diagnosed at advanced stages when treatment options are limited and outcomes are significantly worse.
Research from medical journals shows that among women aged 65 and older—many of whom stopped screening—a disproportionate number present with late-stage cervical cancer. In the United States, women 65 and older account for more than 20% of new cases of cervical cancer and around 37% of deaths from the disease.
The problem? Many never had adequate screening to begin with.
Stage at Diagnosis Matters
Studies examining cervical cancer stage at diagnosis reveal concerning patterns. Women who never received regular screening are significantly more likely to be diagnosed with stage II-IV disease compared to those who followed screening guidelines.
Late-stage diagnosis means the cancer has spread beyond the cervix to nearby tissues, lymph nodes, or distant organs. Treatment becomes more aggressive, side effects more severe, and survival rates drop dramatically.
| Cancer Stage | Description | 5-Year Survival Rate |
|---|---|---|
| Stage I (Early) | Cancer confined to cervix | Over 90% |
| Stage II | Spread beyond cervix but not to pelvic wall | Approximately 60-70% |
| Stage III | Spread to pelvic wall or lower vagina | Approximately 30-40% |
| Stage IV (Advanced) | Spread to bladder, rectum, or distant organs | Less than 20% |
Who’s at Highest Risk for Never Screening
Research from the CDC using 2015 National Health Interview Survey data revealed that only 81.1% of eligible women aged 21-65 were up to date with cervical cancer screening recommendations—falling short of the Healthy People 2020 objective of 93%.
That means nearly 1 in 5 women weren’t getting screened as recommended.
Interestingly, in a 2012 study of women with no cervical cancer screening in the past 5 years, nearly 70% had health insurance and a regular doctor or health care provider. This suggests barriers beyond just access to care.
Common Barriers to Screening
CDC research has identified both financial and nonfinancial barriers that prevent women from getting screened:
- Lack of awareness about screening importance
- Belief that screening isn’t necessary without symptoms
- Fear of the procedure or embarrassment
- Not being sexually active (misconception that screening isn’t needed)
- Previous negative healthcare experiences
- Confusion about screening guidelines and intervals
- Time constraints and difficulty scheduling
Research from 2024 examining screening uptake found that 25.1% of women in a nationally representative sample had never been screened for cervical cancer. Logistic regression models identified significant disparities based on sociodemographic characteristics and psychosocial factors.
Studies also show concerning patterns: Black women had lower likelihood of preferring at-home self-sampling options compared to White women. Women who reported experiencing prejudice or discrimination in medical care settings showed higher preference for at-home collection.
The Myth That Virgins Don’t Need Screening
One dangerous misconception deserves special attention: the belief that women who aren’t sexually active don’t need Pap smears.
This isn’t entirely accurate.
While HPV is primarily transmitted through sexual contact, cervical cancer screening guidelines recommend that all individuals with a cervix start getting Pap tests at age 21, regardless of sexual activity status.
Why? Several reasons:
First, HPV transmission can occur through sexual contact that doesn’t involve intercourse. Second, healthcare providers establish baseline screening and build the habit of regular preventive care. Third, individuals may not accurately recall or report all types of sexual contact.
That said, the American College of Obstetricians and Gynecologists acknowledges that for individuals who have never been sexually active, screening may be deferred after discussion with a healthcare provider. But this decision should be made with medical guidance, not assumed.
Current Screening Guidelines
Understanding when and how often to get screened is critical. Confusion about guidelines has been identified as one barrier to adequate screening.
The CDC outlines clear recommendations as of 2025:
| Age Group | Recommended Screening | Frequency |
|---|---|---|
| Under 21 | No screening needed | N/A |
| 21-29 | Pap test only | Every 3 years |
| 30-65 | Pap test alone, HPV test alone, or co-testing (both) | Every 3 years (Pap), every 5 years (HPV or co-test) |
| Over 65 | May stop if adequate prior screening and no high-risk factors | Discuss with provider |
These guidelines have evolved over time. Annual Pap smears are no longer recommended for most women because research showed that cervical cancer develops slowly enough that less frequent screening is both safe and effective.
But less frequent doesn’t mean never.
Why Screening Intervals Changed
The shift from annual to every-three-years screening for younger women and every-five-years for HPV testing or co-testing reflects improved understanding of cervical cancer development.
Based on a study that included more than 1 million women, researchers at the National Institutes of Health determined that a negative test for human papillomavirus (HPV) compared to a negative Pap test provides greater safety against future risk of cervical cancer. This is why HPV testing alone is now an acceptable primary screening option for women 30 and older.
However, these extended intervals assume regular adherence. Skipping multiple screening cycles or never screening at all eliminates the safety net entirely.
What Happens During Undetected Cancer
When cervical cancer develops without detection, symptoms eventually appear—but often not until the disease has advanced.
Early-stage cervical cancer typically causes no symptoms. This is why screening is so critical.
As cancer progresses, symptoms may include:
- Abnormal vaginal bleeding (between periods, after menopause, after intercourse)
- Unusual vaginal discharge
- Pelvic pain
- Pain during intercourse
- Heavier or longer menstrual periods
By the time these symptoms prompt a medical visit, the cancer may already be at an advanced stage.
Treatment for advanced cervical cancer is far more intensive than treatment for precancerous changes detected through screening. Early precancerous lesions might be treated with simple procedures like cryotherapy or loop electrosurgical excision.
Advanced cancer requires combinations of surgery, radiation, and chemotherapy—with significant impacts on quality of life, fertility, and survival.
The Preventability Factor
Here’s what makes skipping Pap smears particularly tragic: cervical cancer is one of the most preventable cancers.
Cervical cancer screening has been hailed as a major public health achievement precisely because it works. Regular screening, combined with HPV vaccination, has the potential to virtually eliminate cervical cancer.
Research examining the impact of screening and HPV vaccination found that early vaccination resulted in a 40% reduction in cervical precancers (cervical intraepithelial neoplasia, or CIN) and more than an 80% reduction in the overall risk of developing the disease. When combined with regular screening, the protective effect multiplies.
But prevention only works if people participate.
Globally, cervical cancer remains among the second most frequent malignancies among women, with a high proportion of cases occurring in resource-limited settings. In the United States and other developed nations, the disease is far less common—a direct result of widespread screening availability.
Choosing not to utilize available screening essentially forfeits this protection.
Special Populations and Risks
Certain groups face higher risks when skipping screening.
Women over 65 who never had adequate screening during their younger years remain at risk. Research shows they cannot safely discontinue screening without documented evidence of previous normal tests.
Some studies suggest catch-up HPV testing for individuals in their late 60s may be worthwhile if prior screening was inadequate. Results from a population-based study conducted in Denmark suggest that ‘catch-up’ HPV testing for individuals ages 65-69 who haven’t had cervical cancer screening for at least 5 years may be worthwhile, with about 62% of women invited undergoing testing within the next year.
Immunocompromised individuals face elevated risk. Those with HIV, transplant recipients, or people taking immunosuppressive medications need more frequent screening than standard guidelines recommend.
Women with a history of cervical precancer or cancer require ongoing surveillance even after treatment.
Emerging Screening Options
Recognition that screening uptake remains below targets has prompted exploration of alternative approaches.
Self-collected HPV testing has emerged as a promising option to expand access. Research published in 2026 found that 61% of participants preferred in-clinic specimen collection for cervical cancer screening, while at-home sample collection appeals to certain groups, particularly those who have experienced discrimination in healthcare settings.
The American College of Obstetricians and Gynecologists has responded to updated guidelines acknowledging the potential of self-collected high-risk HPV testing while emphasizing the need for proper infrastructure to connect people to follow-up testing and treatment when results are abnormal.
These innovations address barriers for some women but don’t eliminate the fundamental need for screening—they just make it more accessible.
The Cost of Avoidance
Beyond health outcomes, never getting screened has broader implications.
Treatment costs for advanced cervical cancer far exceed the cost of regular screening and early intervention. The economic burden includes not just direct medical expenses but lost productivity, disability, and premature death.
But the human cost matters most.
According to the CDC, cervical cancer results in significant mortality globally, with prevention and screening recognized as critical public health priorities.
In the United States, where screening is widely available, these deaths are largely preventable.
Overcoming Screening Barriers
For women who have avoided screening, reengaging with healthcare is critical.
If fear or embarrassment has been a barrier, discussing concerns with a healthcare provider can help. Many clinics now offer options to make the experience more comfortable.
If confusion about guidelines has caused delays, a straightforward conversation can clarify individual screening needs based on age and history.
If access has been the issue, community health centers, Federally Qualified Health Centers, and programs like the National Breast and Cervical Cancer Early Detection Program provide screening services regardless of ability to pay.
The key is taking that first step—or in this case, scheduling that overdue appointment.
Frequently Asked Questions
Yes. Early-stage cervical cancer typically causes no symptoms, which is exactly why screening is critical. Symptoms usually don’t appear until cancer has advanced to later stages. Absence of symptoms doesn’t mean absence of disease.
Current CDC guidelines recommend starting Pap tests at age 21 regardless of sexual activity. While HPV is sexually transmitted and risk is lower without sexual contact, screening establishes preventive care habits and provides baseline assessment. Individuals who have never been sexually active should discuss their specific situation with a healthcare provider.
The National Cancer Institute found that the percentage of women overdue for screening has been increasing. If overdue, schedule an appointment as soon as possible. A healthcare provider may recommend immediate screening and determine appropriate follow-up intervals based on age, screening history, and risk factors. It’s never too late to start.
For women aged 30-65, HPV testing alone is an acceptable primary screening option according to current guidelines. Based on a study that included more than 1 million women, researchers at the National Institutes of Health determined that a negative test for human papillomavirus (HPV) compared to a negative Pap test provides greater safety against future cervical cancer risk. However, women aged 21-29 should receive Pap tests, not HPV tests alone. Discuss options with a healthcare provider.
Women over 65 may discontinue screening if they’ve had adequate prior screening (three consecutive negative Pap tests or two consecutive negative co-tests within the past 10 years, with the most recent test within 5 years) and no history of moderate or severe abnormal cells or cervical cancer. However, women who never had adequate screening should continue. More than 20% of new cervical cancer cases occur in women over 65.
No. While HPV vaccination reduces cervical precancers by approximately 40% according to 2025 research, it doesn’t protect against all cancer-causing HPV types. Vaccinated individuals still need regular screening according to age-based guidelines. The combination of vaccination and screening provides the strongest protection.
Schedule screening immediately. A healthcare provider will likely recommend co-testing (both Pap and HPV test) to establish baseline information. Based on results, appropriate follow-up will be determined. Starting screening later is far better than never screening at all, especially since cervical cancer develops slowly and early detection dramatically improves outcomes.
The Bottom Line
Never getting a Pap smear removes the single most effective tool for preventing cervical cancer and detecting it early when treatment is most successful.
The consequences range from undetected precancerous changes that progress to invasive cancer, to late-stage diagnoses with survival rates dropping from over 90% to less than 70% or lower depending on stage.
Cervical cancer is highly preventable. The screening tests are proven, effective, and widely available.
If screening has been delayed or avoided, the data is clear: the risks of skipping far outweigh any discomfort or inconvenience of the test itself.
Schedule that appointment. Your future self will thank you.