
Quick Summary: Taking too much iron can cause acute iron poisoning with symptoms ranging from gastrointestinal distress to organ failure and death. Chronic iron overload, whether from excessive supplementation or genetic conditions like hemochromatosis, leads to iron accumulation in vital organs including the liver, heart, and pancreas, causing progressive damage through oxidative stress and potentially life-threatening complications.
Iron is essential for life. The body needs this mineral to produce hemoglobin, the protein in red blood cells that transports oxygen throughout the body.
But here’s the thing—too much iron becomes toxic fast.
Unlike other nutrients that the body can easily excrete, iron has no natural elimination mechanism. When excess iron accumulates, it triggers a cascade of damaging reactions. According to medical research including StatPearls, iron generates reactive oxygen species that cause oxidative stress, cellular damage, and progressive organ dysfunction.
So what exactly happens when someone takes too much iron? The answer depends on whether the exposure is acute or chronic.
Understanding Iron Toxicity: Two Distinct Conditions
Iron toxicity manifests in two fundamentally different ways. Acute iron poisoning occurs when someone ingests a dangerous amount of iron supplements in a short period. Chronic iron overload develops gradually as iron deposits accumulate in tissues over months or years.
The distinction matters because the symptoms, dangers, and treatments differ significantly.
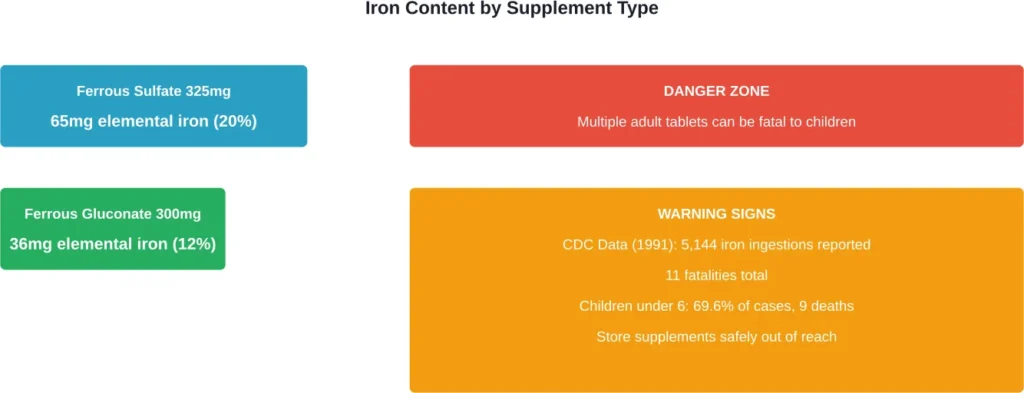
According to StatPearls and LiverTox sources, a 325-mg ferrous sulfate tablet contains approximately 65 mg of elemental iron (20%). A 300-mg ferrous gluconate tablet contains 36 mg (12%) elemental iron. This variation in elemental iron content affects toxicity risk.
How Much Iron Is Too Much?
Toxicity thresholds vary by age and individual factors, but general guidelines exist.
According to CDC data from 1991, poison control centers in the United States reported 5,144 ingestions of iron supplements, with 11 fatalities. Children aged less than 6 years accounted for 69.6% of ingestions and nine of the deaths.
For children, ingestion of adult iron supplements poses extreme danger. Even a handful of tablets can be lethal for a toddler.
Acute Iron Poisoning: The Five Stages
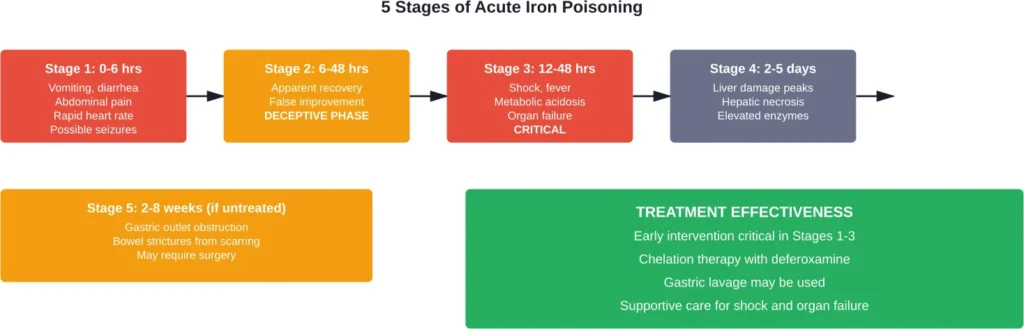
According to the Merck Manuals, acute iron poisoning progresses through five distinct stages. Understanding these stages helps recognize the emergency and guides treatment.
Stage 1: Initial Gastrointestinal Phase (0-6 Hours)
Symptoms appear within six hours of ingestion. Vomiting, sometimes with blood, signals the corrosive effects of iron on the stomach lining. Diarrhea, abdominal pain, irritability, and drowsiness follow.
In severe cases, rapid breathing, elevated heart rate, coma, unconsciousness, or seizures can develop during this initial phase.
The gastrointestinal symptoms result from iron’s direct corrosive action on the mucosa. But that’s just the beginning.
Stage 2: Apparent Recovery (6-48 Hours)
Here’s where iron poisoning gets deceptive. The patient’s condition appears to improve. Symptoms may resolve temporarily, creating a false sense of security.
This latent period doesn’t mean the danger has passed. Iron continues absorbing into the bloodstream, and cellular damage progresses silently.
Stage 3: Systemic Toxicity (12-48 Hours)
The third stage brings life-threatening complications. Very low blood pressure (shock), fever, bleeding, jaundice, liver failure, and seizures can develop rapidly.
According to NIH case reports, metabolic acidosis and organ failure characterize this critical phase. One reported case showed a patient who initially improved after treatment, only to deteriorate within 24 hours with severe vomiting and rapid clinical decline requiring reintubation.
Stage 4: Hepatotoxicity (2-5 Days)
Liver damage peaks during this phase. Elevated liver enzymes, hepatic necrosis, and potential liver failure emerge as iron-induced oxidative stress overwhelms hepatocytes.
Stage 5: Delayed Consequences (2-8 Weeks)
Survivors may develop gastric outlet obstruction or bowel strictures weeks after the acute event. Scarring from the initial corrosive damage can narrow the digestive tract, requiring surgical intervention.
Chronic Iron Overload: The Silent Destroyer
Chronic iron overload develops differently than acute poisoning. Instead of a sudden toxic event, iron accumulates gradually in organs over time.
The most common cause is hereditary hemochromatosis, a genetic condition affecting iron regulation. Hereditary hemochromatosis, an autosomal recessive disorder, disrupts the body’s ability to regulate iron absorption, leading to systemic iron accumulation.
Secondary causes include repeated blood transfusions, chronic hemolysis, and excessive dietary intake over extended periods.
How Iron Damages Organs
Excess iron doesn’t simply sit inert in tissues. It actively generates reactive oxygen species through Fenton chemistry, creating oxidative stress that damages cellular components.
The liver typically bears the brunt of iron accumulation. Hepatic iron deposits progress from simple steatosis to fibrosis and eventually cirrhosis. According to StatPearls, iron promotes cellular damage and progressive organ dysfunction through this oxidative mechanism.
But the damage doesn’t stop at the liver.
Iron deposits in the heart cause restrictive cardiomyopathy and arrhythmias. Pancreatic accumulation leads to diabetes mellitus—sometimes called “bronze diabetes” due to the skin discoloration that accompanies hemochromatosis. Endocrine glands suffer dysfunction, and joints develop arthropathy.
Symptoms of Chronic Iron Overload
Early symptoms are often vague and nonspecific. Fatigue, weakness, and joint pain may be dismissed or attributed to other causes.
As iron accumulation progresses, more distinctive signs emerge:
- Bronze or gray skin discoloration
- Abdominal pain and liver enlargement
- Loss of libido and testicular atrophy
- Heart rhythm abnormalities
- Diabetes symptoms (increased thirst, urination)
- Arthritis, particularly in the hands
Cleveland Clinic notes that hemochromatosis can damage organs over time, but the condition is treatable when detected early.
Diagnosing Iron Toxicity and Overload
Diagnosis approaches differ for acute versus chronic conditions.
Acute Iron Poisoning Diagnosis
Medical teams rely on patient history (reported ingestion), clinical presentation, and laboratory tests. Serum iron levels provide direct measurement of circulating iron.
According to case reports from medical literature, one adult patient presented with serum iron levels of 185 μg/dL, serum ferritin of 692 ng/dL, and total iron binding capacity of 90 μg/dL. Blood gas analysis revealed severe metabolic acidosis.
Radiography may visualize iron tablets in the gastrointestinal tract, as iron is radiopaque.
Chronic Iron Overload Diagnosis
Screening begins with serum ferritin and transferrin saturation. Elevated ferritin suggests increased iron stores, though inflammation can also raise this marker.
Transferrin saturation above 45% warrants further investigation. Genetic testing for HFE mutations (C282Y and H63D) confirms hereditary hemochromatosis.
Liver biopsy or MRI can quantify hepatic iron concentration in ambiguous cases.
Treatment: How Medical Teams Respond
Treatment urgency and methods depend on whether the situation involves acute poisoning or chronic overload.
Acute Iron Poisoning Treatment
Time is critical. According to Poison.org, immediate steps include contacting poison control and seeking emergency care.
In the emergency department, treatments may include:
- Gastric lavage to remove unabsorbed iron from the stomach
- Whole bowel irrigation with polyethylene glycol solution
- Chelation therapy with deferoxamine, which binds iron and allows urinary excretion
- Supportive care for shock, including IV fluids and vasopressors
- Correction of metabolic acidosis
- Treatment of organ failure (dialysis for kidney failure, ventilatory support for respiratory failure)
Deferoxamine chelation specifically targets free iron, converting it to ferrioxamine that the kidneys can eliminate. According to StatPearls, this represents the primary antidote for severe iron toxicity.
Chronic Iron Overload Treatment
Therapeutic phlebotomy—regular blood removal—represents the standard treatment for hemochromatosis. Removing blood forces the body to use stored iron to produce new red blood cells.
Initially, phlebotomy occurs weekly until ferritin levels normalize. Maintenance phlebotomy continues every 2-4 months to prevent reaccumulation.
For patients who can’t tolerate phlebotomy, chelation therapy with deferasirox or deferoxamine provides an alternative.
Dietary modifications play a supporting role. Avoiding vitamin C supplements (which enhance iron absorption), limiting alcohol, and reducing iron-rich foods help manage the condition.
| Condition | Primary Treatment | Mechanism | Duration |
|---|---|---|---|
| Acute Iron Poisoning | Deferoxamine chelation | Binds free iron for urinary excretion | 24-48 hours typically |
| Hemochromatosis | Therapeutic phlebotomy | Removes iron-containing blood | Lifelong maintenance |
| Transfusion Overload | Deferasirox chelation | Oral chelator, daily dosing | Ongoing as needed |
| Severe Acute Cases | Supportive ICU care | Manages organ failure, shock | Days to weeks |
Who’s at Highest Risk?
Several groups face elevated risk for iron toxicity or overload.
Young children top the list for acute poisoning. The CDC documented that children under 6 accounted for nearly 70% of iron ingestion cases. Toddlers exploring their environment can mistake colorful supplements for candy.
Adults with hereditary hemochromatosis face chronic overload risk. Individuals of northern European descent carry higher rates of HFE mutations.
Patients receiving repeated blood transfusions—for conditions like thalassemia or sickle cell disease—accumulate iron from transfused red blood cells. Each unit of transfused blood contains approximately 200-250 mg of iron, and the body has no efficient elimination route.
People taking iron supplements without medical supervision risk gradual overload, especially if they don’t actually have iron deficiency.
Iron and Cancer: The Concerning Connection
Research suggests excess iron may increase cancer risk, though the relationship remains complex.
Iron’s ability to generate reactive oxygen species can damage DNA, potentially initiating carcinogenic mutations. Observational studies have linked elevated iron stores to increased colorectal cancer risk.
Research suggests iron’s harmful effects in high amounts include raising infection and cancer risk, with immune and oxidative stress mechanisms providing biological plausibility. The oxidative stress mechanism provides biological plausibility for this association.
That said, more research is needed to establish definitive causal relationships and identify specific risk thresholds.
Iron and Infection Risk
Many bacteria and pathogens require iron for growth and virulence. Excess iron in the bloodstream may enhance certain infections.
The body normally sequesters iron during infection as a defense mechanism. Elevated circulating iron undermines this protective response, potentially worsening infectious outcomes.
Conditions causing chronic iron overload have been associated with increased susceptibility to specific pathogens, including Vibrio vulnificus, Yersinia enterocolitica, and certain fungal infections.
Prevention: Keeping Iron Levels Safe
Most people get adequate iron from diet alone. Red meat, poultry, fish, legumes, and fortified cereals provide sufficient amounts.
Supplementation should occur only when medically indicated—diagnosed iron deficiency or specific conditions like pregnancy that increase requirements.
For households with children, storage matters enormously. Keep iron supplements in child-resistant containers, stored out of reach and sight. Following safety guidance, closing child-resistant packages tightly after each use and storing iron supplements out of reach prevents accidental access.
Adults should avoid self-prescribing high-dose iron without laboratory confirmation of deficiency. Routine monitoring of ferritin and transferrin saturation helps catch overload early in at-risk individuals.
For those with hereditary hemochromatosis, early diagnosis through genetic screening of family members enables preventive treatment before organ damage occurs.
Frequently Asked Questions
For children, even small amounts from adult supplements can be dangerous. Case reports document fatal poisoning in toddlers from ingestion of adult iron tablets. For adults, doses above 20 mg/kg of elemental iron can cause toxicity, with severe poisoning occurring at higher doses. Individual tolerance varies based on body weight and other factors.
The first signs typically appear within 6 hours and include vomiting (sometimes with blood), diarrhea, severe abdominal pain, and irritability. According to the Merck Manuals, rapid heart rate and breathing may also occur. These symptoms indicate Stage 1 of acute iron poisoning and require immediate medical attention.
Recovery is possible with prompt treatment. Early chelation therapy with deferoxamine and supportive care significantly improve outcomes. However, NIH case reports document fatal cases even with treatment, particularly when ingestion involves very high doses or treatment is delayed. The deceptive Stage 2 improvement period makes continued monitoring essential.
Chronic iron overload develops gradually over months or years, typically from genetic conditions like hemochromatosis or repeated blood transfusions. Symptoms are subtle initially—fatigue, joint pain, skin discoloration. Acute poisoning occurs suddenly after ingesting toxic amounts of iron supplements, causing severe gastrointestinal symptoms and rapid progression to organ failure without treatment.
Hemochromatosis is a genetic disorder that disrupts iron regulation, causing the body to absorb and store too much iron. According to Cleveland Clinic, excess iron accumulates in organs including the liver, heart, and pancreas, causing progressive damage. It’s treatable through regular therapeutic phlebotomy, which removes iron-containing blood to reduce body stores.
Only take iron supplements if diagnosed with iron deficiency through blood tests or if recommended by a healthcare provider for specific conditions like pregnancy. According to dietary guidelines from the Office of Dietary Supplements and food sources, most people obtain adequate iron from food. Unnecessary supplementation risks toxicity and organ damage over time.
Contact Poison Control immediately at 1-800-222-1222 or use the webPOISONCONTROL online tool. If the person collapses, has a seizure, trouble breathing, or can’t be awakened, call 911 immediately. According to Poison.org, both resources provide free, expert, confidential guidance. Do not wait for symptoms to appear—iron poisoning requires rapid intervention.
The Bottom Line
Iron toxicity represents a serious medical emergency that demands immediate attention. The difference between life-threatening poisoning and full recovery often comes down to how quickly treatment begins.
For acute ingestions, recognizing the five-stage progression and seeking emergency care during Stage 1 provides the best outcomes. Don’t be fooled by the apparent improvement in Stage 2—continued medical monitoring is essential.
Chronic iron overload, though slower to develop, causes equally serious organ damage. Early detection through screening, particularly for those with family history of hemochromatosis, enables preventive intervention before irreversible complications occur.
Store supplements safely. Never self-prescribe iron without laboratory confirmation of deficiency. And if you suspect iron poisoning in yourself or someone else, contact emergency services or Poison Control immediately.
Your organs don’t have a backup plan for dealing with excess iron. Prevention and rapid response remain the most effective strategies for avoiding the devastating consequences of iron toxicity.