
Quick Summary: While true rib dislocation is extremely rare due to strong ligament attachments, the lower ribs (8-12) can experience subluxation—a partial displacement causing slipping rib syndrome. This condition affects about 5% of chest wall pain cases and involves abnormal movement of rib cartilage, not complete dislocation.
The short answer? Complete rib dislocation is extraordinarily rare in typical circumstances. What most people experience—and what doctors commonly treat—is rib subluxation, a partial displacement that causes significant discomfort without full joint separation.
Here’s the thing though: the term “dislocated rib” gets thrown around casually, but it doesn’t accurately describe what’s actually happening in most cases. Understanding the difference matters for proper diagnosis and treatment.
Understanding Rib Anatomy and Joint Connections
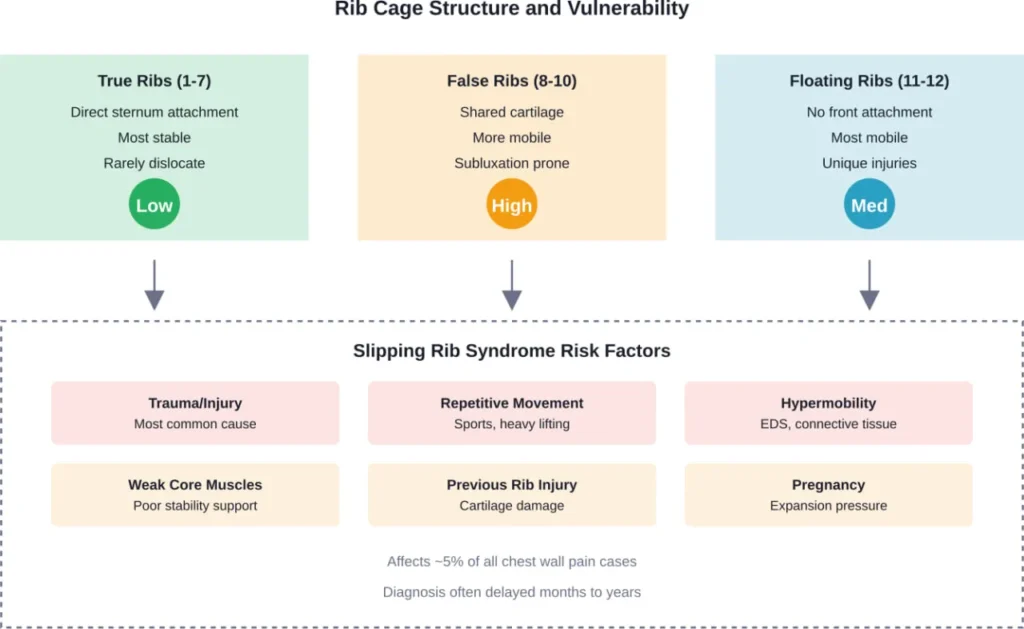
Your rib cage contains 12 pairs of ribs, each with different attachment patterns. The upper seven ribs—called “true ribs”—connect directly to your sternum (breastbone) through individual cartilage pieces. These connections are incredibly stable.
Ribs 8 through 10, known as “false ribs,” share cartilage connections. They attach to the rib above rather than directly to the sternum. This shared connection creates more mobility but also more vulnerability.
The bottom two ribs (11 and 12) float freely without front attachments. At the back, all ribs connect to thoracic vertebrae through costovertebral joints, which are reinforced by strong ligaments.
According to research published in Cureus, the thoracic cage provides between 30-40% of thoracic spine stiffness, with rib-joint stiffness greatest at T2 and weakest at T10, making these connections structurally critical.
Dislocation vs. Subluxation: What’s Actually Happening
A true dislocation means complete separation of joint surfaces. For ribs, this requires catastrophic trauma—think high-speed car accidents or severe crush injuries. The ligaments holding ribs in place are remarkably strong.
Subluxation, on the other hand, is a partial dislocation where joint surfaces lose their normal relationship but maintain some contact. This is what happens in slipping rib syndrome, also called interchondral subluxation or Cyriax syndrome.
Recent data suggests that slipping rib syndrome accounts for about 5% of all cases of chest wall pain. Unfortunately, given the vagueness of symptoms and lack of clear radiologic evidence, patients can sometimes see physicians for months to years before obtaining a correct diagnosis, as noted in a 2020 comprehensive review published in Psychopharmacology Bulletin.
What Is Slipping Rib Syndrome?
Slipping rib syndrome occurs when the cartilage connecting your eighth, ninth, or tenth ribs becomes damaged or loose. These ribs normally share cartilage attachments, but when that cartilage slips or moves abnormally, it causes pain.
In ultrasound studies of costotransverse joint inflammatory disease, the most frequently affected limb was the non-dominant one (80% of cases). In ultrasound studies of costotransverse joint inflammation, 73.3% of enrolled patients were female.
But wait—there’s another type of rib injury that gets confused with slipping rib syndrome. Costovertebral joint dislocations involve the back attachments of ribs to the spine. These are even rarer and usually result from severe trauma.
Common Symptoms to Watch For
People with slipping rib syndrome typically experience:
- Sharp, intermittent pain in the lower chest or upper abdomen
- Pain that worsens with movement, deep breathing, or coughing
- A clicking, popping, or slipping sensation
- Tenderness when pressing on the affected area
- Pain that may radiate to the back or shoulder
The pain can be severe enough to interfere with daily activities. Many patients undergo extensive testing—including imaging for heart, lung, or digestive problems—before receiving an accurate diagnosis.
Causes and Risk Factors
Several factors can lead to rib subluxation or increased rib mobility:
Trauma and injury top the list. Direct blows to the chest, falls, or car accidents can damage rib cartilage. Even seemingly minor injuries can cause problems that develop over time.
Repetitive strain affects athletes and manual laborers. Activities involving twisting, reaching, or heavy lifting stress the interchondral joints repeatedly. Sports like rowing, swimming, and contact sports carry higher risk.
Hypermobility disorders make some people more vulnerable. Conditions like Ehlers-Danlos Syndrome (EDS) affect connective tissue, making joints throughout the body—including rib attachments—more prone to subluxation.
Physical therapists working with hypermobile patients report that rib subluxations are particularly common in this population, though most medical literature historically dismissed the possibility.
| Risk Factor | Mechanism | Common In |
|---|---|---|
| Direct trauma | Cartilage damage or tear | Accidents, falls, sports injuries |
| Repetitive motion | Gradual cartilage wear | Athletes, manual laborers |
| Hypermobility | Weak connective tissue | EDS, joint hypermobility syndrome |
| Pregnancy | Rib cage expansion, hormone effects | Third trimester, postpartum |
| Previous rib injury | Weakened healing cartilage | Post-fracture, post-surgery |
Diagnosis: Why It Takes So Long
Standard imaging—X-rays, CT scans, even MRI—often appears completely normal. Rib cartilage doesn’t show up well on these tests, and the subluxation may only occur with certain movements.
Doctors typically rely on physical examination. The “hooking maneuver” is diagnostic: the examiner hooks fingers under the rib margin and pulls forward. If this reproduces the pain and clicking sensation, slipping rib syndrome is likely.
Ultrasound evaluation is gaining recognition as a diagnostic tool. It can visualize cartilage movement and inflammation in real-time, though it requires an experienced operator.
Some patients receive diagnostic nerve blocks. Injecting local anesthetic into the affected area temporarily relieves pain if slipping rib syndrome is the culprit.
Treatment Options That Actually Work
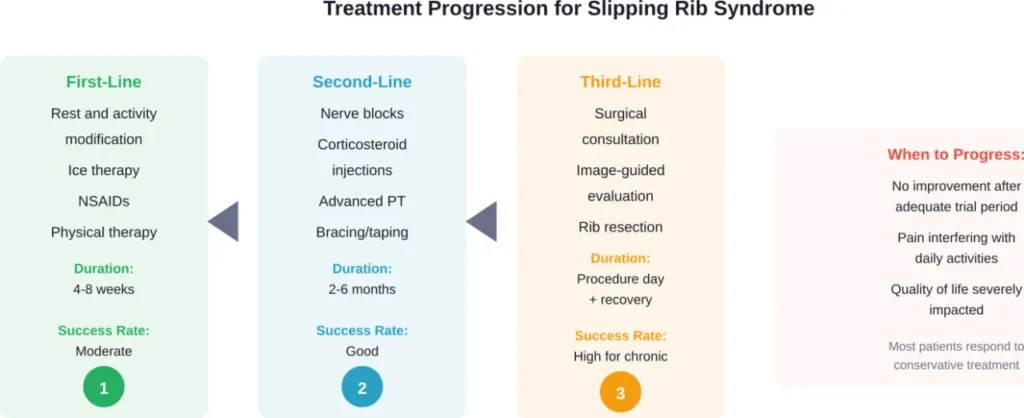
Conservative management succeeds for many patients. Rest, ice application, and avoiding aggravating movements allow inflamed cartilage to settle down. Physical therapy strengthens core muscles that support the rib cage.
Anti-inflammatory medications reduce pain and swelling. Some patients benefit from intercostal nerve blocks or injections of corticosteroids directly into the affected joint.
When Surgery Becomes Necessary
For chronic, debilitating cases that don’t respond to conservative treatment, surgical options exist. Rib resection removes the affected rib segment and its cartilage attachment.
Thoracic surgeons have developed specialized techniques for this procedure. WVU Medicine reported cases of patients who experienced pain for 10 or more years, seen multiple doctors, and undergone unnecessary procedures like appendectomies before receiving proper diagnosis and treatment.
In reported surgical cases, operative time was 57 minutes in one procedure and 59 minutes in another, with estimated blood loss of 100 mL in the first operation and 20 mL in the second. Patients often experience significant pain relief and improved quality of life postoperatively.
True Costovertebral Dislocation: The Rarer Injury
While slipping rib syndrome involves front rib attachments, costovertebral joint dislocations affect where ribs connect to the spine. These injuries are extremely uncommon.
Medical literature contains only scattered case reports. One describes a 24-year-old man admitted after a high-speed car collision with costovertebral joint dislocation. Another documents left fourth and sixth rib dislocations following blunt thoracic trauma.
These injuries require significant force and often accompany other serious trauma. They can potentially compress the spinal cord or major blood vessels, making them medical emergencies requiring immediate imaging and intervention.
When to Seek Medical Attention
Certain symptoms demand immediate evaluation:
- Severe chest pain, especially if sudden or crushing
- Difficulty breathing or shortness of breath
- Chest pain accompanied by fever, cough, or illness symptoms
- Pain radiating to the jaw, neck, or left arm
- Visible deformity of the chest wall
For less urgent symptoms—persistent clicking sensation, pain with movement, or localized tenderness—schedule an appointment with a primary care physician or orthopedic specialist. Early diagnosis prevents unnecessary testing and gets treatment started sooner.
Prevention Strategies
While accidents happen, certain measures reduce risk:
Core strengthening provides better support for the rib cage. Exercises targeting abdominal and back muscles create stability that protects rib attachments during movement.
Proper lifting technique matters. Bending at the knees rather than twisting at the waist reduces strain on intercostal joints. This applies whether lifting weights at the gym or moving furniture at home.
Athletes should gradually increase training intensity. Sudden jumps in volume or load stress connective tissues before they adapt. Progressive overload allows cartilage and ligaments to strengthen gradually.
| Prevention Strategy | How It Helps | Best For |
|---|---|---|
| Core strengthening | Stabilizes rib cage during movement | Everyone, especially athletes |
| Proper lifting mechanics | Reduces twisting forces on ribs | Manual laborers, gym-goers |
| Gradual training progression | Allows tissue adaptation | Athletes, fitness enthusiasts |
| Posture awareness | Maintains optimal rib alignment | Desk workers, everyone |
| Protective equipment | Prevents direct trauma | Contact sport athletes |
Living With Hypermobility Disorders
Patients with Ehlers-Danlos Syndrome or other hypermobility conditions face unique challenges. Joint instability throughout the body—including rib attachments—creates ongoing vulnerability.
Physical therapy focuses on building muscular support to compensate for loose ligaments. Proprioceptive training improves body awareness, helping patients avoid positions that trigger subluxations.
Many hypermobile patients find that consistent, gentle exercise maintains better stability than complete rest. Swimming and yoga often work well, though modifications may be necessary to avoid problematic positions.
FAQs
Yes, this is exactly what happens in slipping rib syndrome. The cartilage attachment slips out of normal position and may return on its own, often with a clicking or popping sensation. This differs from true dislocation, which requires medical intervention to relocate.
With conservative treatment, most cases improve within 4-8 weeks. However, complete healing of damaged cartilage may take several months. Chronic cases that have persisted for years may require more intensive treatment or surgical intervention.
Standard X-rays typically appear normal in slipping rib syndrome because cartilage doesn’t show up well on these images. The subluxation may only occur with specific movements that aren’t captured during imaging. Ultrasound or physical examination are more reliable diagnostic tools.
While not life-threatening, slipping rib syndrome can significantly impact quality of life. The pain can be severe and debilitating, interfering with work, exercise, and daily activities. Proper diagnosis and treatment are important for long-term relief.
Most patients describe sharp, intermittent pain in the lower chest or upper abdomen that worsens with movement, deep breathing, or coughing. Many feel a distinct clicking, popping, or slipping sensation. The area is usually tender to touch, and pain may radiate to the back or shoulder.
Some patients report relief from chiropractic manipulation or physical therapy techniques. However, if cartilage is significantly damaged, manual therapy alone may not provide lasting improvement. A comprehensive treatment approach often works best.
Mild cases occasionally resolve without specific treatment, especially if the triggering activity is stopped. However, many cases persist or recur without intervention. Early treatment prevents cartilage damage from worsening and improves outcomes.
Conclusion
So, can ribs actually dislocate? Complete dislocation is exceptionally rare, requiring extreme trauma. What most people experience is rib subluxation—partial displacement that’s uncomfortable but treatable.
Slipping rib syndrome affects about 5% of chest wall pain cases yet often goes undiagnosed for extended periods. The condition involves abnormal movement of lower rib cartilage, not true dislocation of bone.
If persistent chest or upper abdominal pain is interfering with your life—especially if accompanied by clicking sensations or pain with movement—consult a healthcare provider familiar with this condition. Early diagnosis leads to faster relief and better outcomes.
Don’t accept months or years of unexplained pain. The right diagnosis makes all the difference between continued suffering and getting back to normal activities. Talk to your doctor about slipping rib syndrome if your symptoms match this pattern.