
Quick Summary: Yes, it is medically possible to vomit fecal matter, a condition known as feculent vomiting or copremesis. This rare and serious phenomenon typically occurs when a complete intestinal obstruction prevents normal digestion, causing intestinal contents to back up into the stomach and be expelled through vomiting. It constitutes a medical emergency requiring immediate treatment.
While it sounds like something from a horror movie, vomiting fecal matter is a documented medical phenomenon. Known in clinical settings as feculent vomiting, copremesis, or stercoraceous vomiting, this condition represents one of the most severe gastrointestinal emergencies.
The reality is unsettling but straightforward: when intestinal contents cannot move forward through the digestive system, they eventually move backward. And yes, that includes material from the lower intestines.
What Is Feculent Vomiting?
Feculent vomiting occurs when the material expelled during vomiting is of fecal origin. This doesn’t necessarily mean someone is vomiting formed stool. Rather, the vomited material contains bacteria and partially digested matter from the lower intestines, giving it a characteristic fecal odor and appearance.
According to medical literature from the National Institutes of Health, this condition is commonly associated with gastrojejunocolic fistula and intestinal obstruction in the ileum. The vomitus typically has a brown color and unmistakable fecal smell due to bacterial overgrowth in the obstructed intestinal segment.
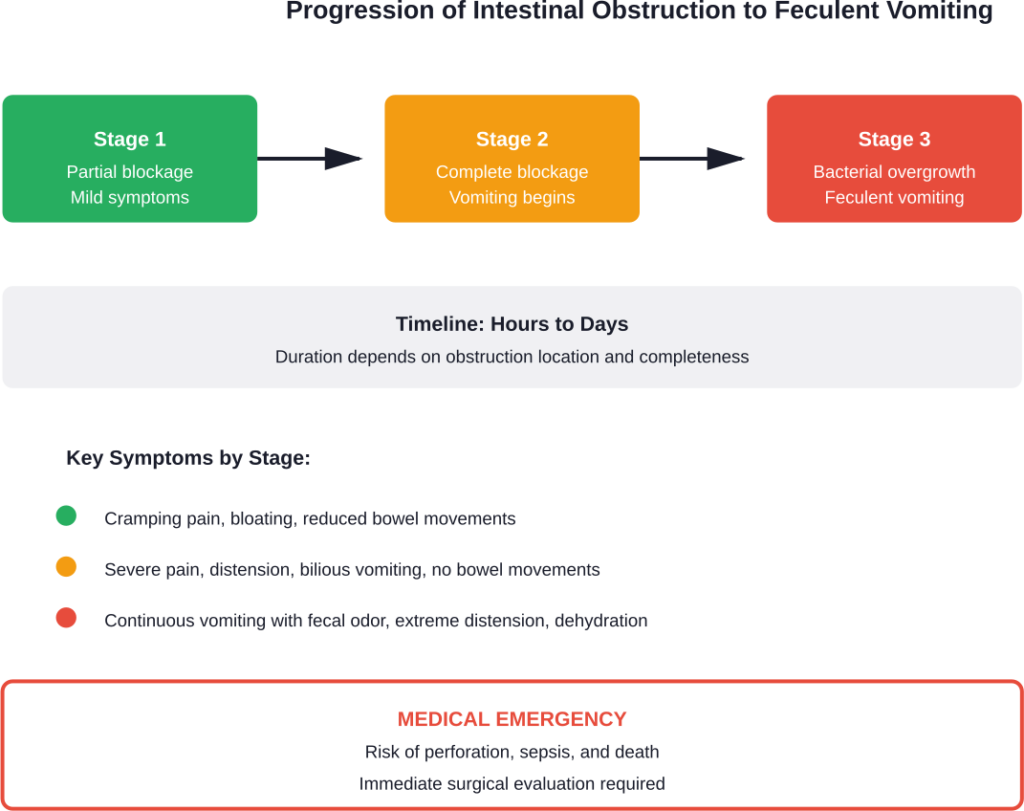
Here’s the thing though—feculent vomiting doesn’t happen suddenly. It’s the end result of progressive intestinal obstruction that has gone untreated.
What Causes Someone to Vomit Fecal Matter?
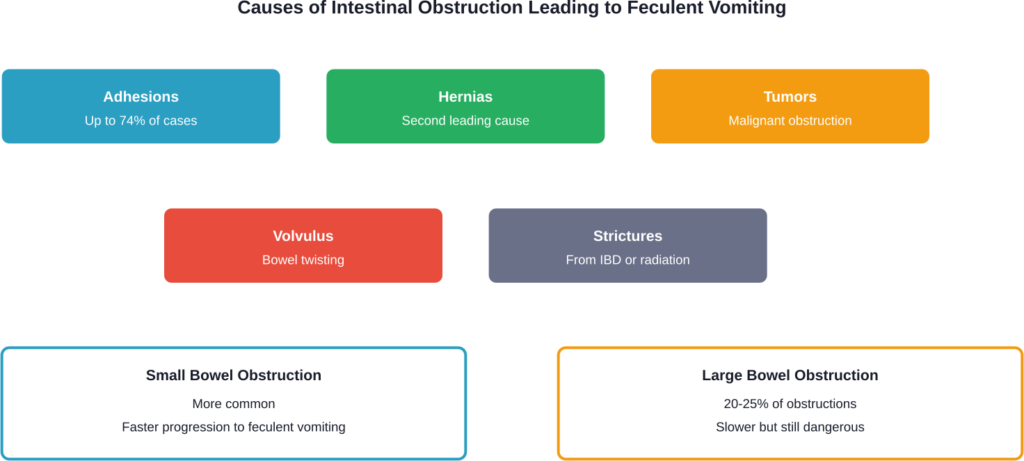
The primary cause of feculent vomiting is mechanical intestinal obstruction. When something physically blocks the intestines, digestive contents accumulate above the blockage. With nowhere else to go, these contents eventually reverse direction.
Small Bowel Obstruction
Small bowel obstruction accounts for the majority of cases leading to feculent vomiting. According to NIH data, postoperative adhesions are the leading cause of small bowel obstruction in developed countries, accounting for up to 74% of cases.
Other causes include hernias, tumors, strictures from inflammatory bowel disease, and intussusception. In adults with intussusception, a neoplasm serves as the lead point in 80-90% of cases.
Large Bowel Obstruction
Large bowel obstructions result in 20 to 25% of all bowel obstructions encountered. These are less likely to cause feculent vomiting initially but can progress to that point if untreated.
Colorectal cancer, diverticular disease, and volvulus are common culprits. Cecal bascule, a rare type of cecal volvulus, has an incidence of 2.8-7.1 per million people per year and accounts for only 1-2% of all large bowel obstructions.
Fecal Impaction
Severe fecal impaction can create functional obstruction. According to research published in Clinical Colon and Rectal Surgery, fecal impaction remains prevalent mostly in pediatric and elderly populations. The condition occurs when hardened fecal matter retained in the large bowel cannot be evacuated by regular peristaltic activity.
Among hospitalized patients, administration of opioid medications in elderly individuals can result in fecal impaction, especially in those with a history of chronic constipation who are bedridden.
Pseudo-Obstruction
Intestinal pseudo-obstruction is characterized by bowel dilation without anatomical obstruction. The National Institute of Diabetes and Digestive and Kidney Diseases recognizes two forms: chronic intestinal pseudo-obstruction and acute colonic pseudo-obstruction (Ogilvie syndrome).
These conditions mimic mechanical obstruction but result from impaired peristalsis or dysregulation of the autonomic nervous system rather than physical blockage.
Warning Signs and Symptoms
Feculent vomiting doesn’t occur in isolation. It’s accompanied by a constellation of symptoms indicating severe intestinal distress.
The classic triad of bowel obstruction includes abdominal pain, vomiting, and abdominal distension. But when obstruction progresses to the point of feculent vomiting, symptoms become more severe.
| Symptom Category | Early Signs | Advanced Signs |
|---|---|---|
| Vomiting | Frequent, after meals | Fecal odor and appearance |
| Abdominal Pain | Cramping, intermittent | Severe, constant |
| Distension | Bloating, fullness | Marked swelling, tightness |
| Bowel Movements | Reduced frequency | Complete obstipation |
| Other | Nausea, decreased appetite | Dehydration, shock |
According to medical case reports, vomiting episodes can become more frequent over a period of 2 days, occurring mostly after meals initially. As obstruction worsens, vomiting becomes continuous regardless of oral intake.
The appearance and smell of the vomitus provide crucial diagnostic clues. Early in obstruction, vomitus may be gastric contents or bile. But as intestinal bacteria proliferate in the stagnant bowel contents above the obstruction, the vomitus takes on a brown color and unmistakable fecal odor.
When Feculent Vomiting Becomes Life-Threatening
Feculent vomiting represents a medical emergency. The presence of fecal vomiting indicates complete or near-complete obstruction that has persisted long enough for significant bacterial overgrowth.
Several complications can rapidly develop. Bowel ischemia occurs when blood supply to the intestinal wall becomes compromised, leading to tissue death. Perforation can result from increased intraluminal pressure or necrotic bowel, causing peritonitis and sepsis.
Dehydration and electrolyte imbalances develop quickly due to fluid sequestration in the dilated bowel and losses through vomiting. According to NIH data on malignant bowel obstruction, the expected median survival of patients with this condition is 1 to 3 months if underlying cancer cannot be treated.
Aspiration of feculent vomitus poses another serious risk, potentially causing chemical pneumonitis or aspiration pneumonia.
Diagnosis and Medical Evaluation
When someone presents with suspected bowel obstruction and feculent vomiting, rapid evaluation is essential. The diagnostic approach combines clinical assessment with imaging studies.
Physical examination reveals abdominal distension, altered bowel sounds (either hyperactive early or absent later), and tenderness. The presence of surgical scars suggests adhesions as a possible cause.
Imaging studies provide definitive diagnosis. Abdominal X-rays can show dilated bowel loops, air-fluid levels, and absence of gas in the distal colon. CT scanning offers more detailed visualization, identifying the obstruction site, underlying cause, and complications like ischemia or perforation.
Laboratory tests assess the degree of dehydration, electrolyte disturbances, and signs of infection or tissue damage. Elevated white blood cell count, lactate levels, and metabolic acidosis may indicate bowel ischemia or perforation.
Treatment Approaches
Treatment of feculent vomiting requires addressing the underlying intestinal obstruction. Conservative management may be attempted in select cases of partial obstruction, but complete obstruction with feculent vomiting typically requires surgical intervention.
Immediate Stabilization
Initial management focuses on stabilization. This includes nothing by mouth (NPO status), nasogastric tube placement for decompression, intravenous fluid resuscitation, and electrolyte correction.
Broad-spectrum antibiotics are initiated if bowel ischemia, perforation, or systemic infection is suspected.
Surgical Intervention
Most cases of complete bowel obstruction causing feculent vomiting require surgery. The specific procedure depends on the underlying cause and extent of bowel damage.
Options include adhesiolysis for adhesive obstruction, hernia repair, bowel resection for ischemic or cancerous segments, and stoma creation if primary anastomosis isn’t safe.
Palliative Management
For patients with malignant bowel obstruction who aren’t surgical candidates, palliative approaches focus on symptom control. According to research in the Canadian Family Physician, gastrointestinal obstructions occur in about 3% to 5% of palliative care patients.
Palliative options include pharmacological management with antiemetics, antisecretory agents, and analgesics. Venting gastrostomy tubes can provide decompression without nasogastric intubation. In select cases, endoscopic stenting may relieve obstruction temporarily.
Prevention and Risk Reduction
While not all causes of intestinal obstruction are preventable, certain measures can reduce risk. Managing chronic constipation aggressively, especially in elderly patients and those on opioid medications, is crucial.
Prompt evaluation of abdominal pain and changes in bowel habits can lead to early diagnosis before complete obstruction develops. For patients with previous abdominal surgery, awareness of adhesion risk and early symptom recognition matters.
Regular colorectal cancer screening allows detection and treatment of lesions before they cause obstruction.
Frequently Asked Questions
Yes, feculent vomiting is a real medical condition where intestinal contents with fecal characteristics are expelled through vomiting. This occurs due to severe intestinal obstruction causing intestinal contents to back up into the stomach. The vomitus contains bacteria and material from the lower intestines, giving it a brown color and fecal odor, though it’s not typically formed stool.
Feculent vomit has a distinctive brown color and an unmistakable fecal odor. The smell comes from bacterial overgrowth in the obstructed bowel segment. The appearance can range from brown liquid to partially digested material mixed with intestinal bacteria. Medical professionals can often identify feculent vomiting immediately based on the characteristic smell alone.
The timeline varies depending on the obstruction’s location and completeness. Proximal small bowel obstructions may progress to feculent vomiting within hours to a couple of days. Distal obstructions take longer, potentially several days. According to medical case reports, vomiting can become more frequent over a period of 2 days before developing fecal characteristics.
Feculent vomiting indicates severe obstruction requiring immediate medical evaluation. While not every case requires surgery, most complete obstructions causing feculent vomiting do. Conservative management may be attempted in carefully selected partial obstruction cases, but the presence of feculent vomiting suggests advanced obstruction that typically needs surgical intervention to prevent life-threatening complications.
Survival depends on the underlying cause and how quickly treatment is provided. For adhesive small bowel obstruction treated promptly, outcomes are generally good. However, according to NIH data, malignant bowel obstruction has a median survival of 1 to 3 months. Complications like perforation and sepsis significantly worsen prognosis, making early intervention critical.
Severe fecal impaction can create functional obstruction that may progress to feculent vomiting in extreme cases. This is most common in elderly, bedridden patients, especially those taking opioid medications. Research shows fecal impaction remains prevalent in pediatric and elderly populations. However, feculent vomiting from constipation alone is rare and typically requires prolonged, severe impaction.
Doctors use imaging studies, particularly CT scans, to identify physical blockages in mechanical obstruction. Pseudo-obstruction shows bowel dilation without anatomical blockage. Clinical history helps—pseudo-obstruction often follows surgery, occurs in critically ill patients, or is associated with medications and metabolic imbalances. According to the National Institute of Diabetes and Digestive and Kidney Diseases, pseudo-obstruction can be acute or chronic and requires ruling out mechanical causes before diagnosis.
The Bottom Line
Feculent vomiting is a real, documented medical condition that occurs when intestinal obstruction progresses to a critical point. While rare, it represents a true gastrointestinal emergency requiring immediate medical intervention.
The key takeaway? Don’t ignore progressive abdominal symptoms. What starts as constipation, bloating, or intermittent cramping can escalate to complete obstruction if underlying causes aren’t addressed.
If you or someone you know experiences persistent vomiting combined with abdominal pain, distension, and inability to pass stool or gas, seek emergency medical care immediately. Early recognition and treatment of bowel obstruction can prevent progression to feculent vomiting and its potentially fatal complications.
Medical advances have improved outcomes for intestinal obstruction, but success depends on prompt diagnosis and appropriate intervention. When it comes to gastrointestinal emergencies, time truly matters.