
Quick Summary: While humans cannot naturally develop three fully-formed breasts, the medical condition polymastia allows for additional breast tissue to appear along the embryonic milk line. This rare condition affects 0.22-6% of the population and typically presents as accessory breast tissue rather than a complete third breast. Medical science confirms that three breasts can exist through this developmental variation or surgical intervention.
The question of whether someone can have three breasts seems like science fiction. But here’s the thing—medical science confirms this is entirely possible through a condition called polymastia.
Polymastia isn’t exactly what most people imagine when they picture a third breast. It’s the presence of supernumerary (extra) breast tissue on the human body, and it’s more common than most realize.
Understanding Polymastia and Accessory Breast Tissue
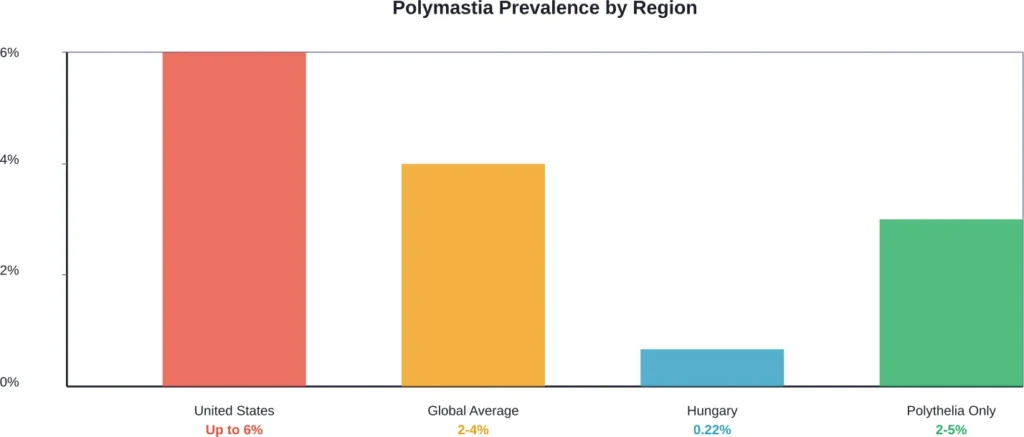
Polymastia refers to the development of additional breast tissue beyond the standard two breasts. According to medical research, this condition affects between 0.22% to 6% of the population, with significant geographic variation, depending on geographic location.
In Hungary, supernumerary breasts affect less than 0.22% of the population. But in the United States, the prevalence jumps to as high as 6%. That’s a significant variation based on regional factors.
The condition develops along what’s called the milk line—an embryonic ridge that extends from the axilla (armpit) to the groin area. During early fetal development around week four of gestation, two parallel lines of glandular tissue form. Most of this tissue regresses before birth, except for the paired masses in the pectoral region that become normal breasts.
When portions of the mammary ridge fail to involute completely, clusters of primordial breast cells persist. These create accessory breast tissue.
Types of Supernumerary Breast Development
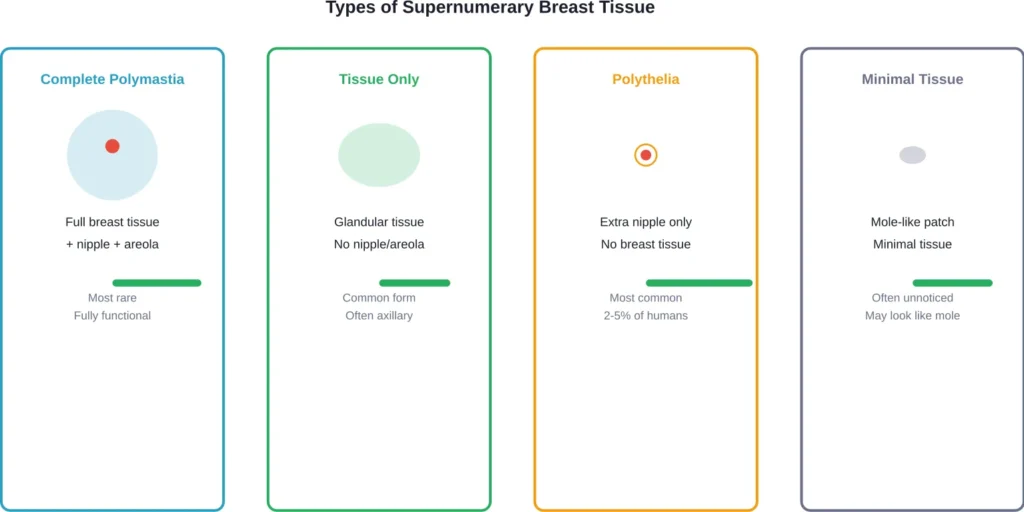
Not all extra breast tissue looks the same. Medical literature identifies several presentations:
- Complete accessory breasts with nipple, areola, and glandular tissue
- Accessory breast tissue without nipple or areola
- Polythelia—extra nipples without breast tissue
- Patch of tissue that resembles a mole or skin tag
According to medical research, polymastia occurs in 2-6% of the population, though prevalence varies by geography and includes both males and females The spectrum ranges from a small mole-like lesion to a fully functional ectopic breast capable of lactation.
Where Extra Breast Tissue Appears
The embryonic milk line determines where accessory breast tissue can develop. This bilateral line extends from slightly beyond the underarm region, tracing down the chest and abdomen, reaching the groin area, and terminating near the inner thighs.
Most supernumerary breast tissue appears along this predictable path. The most common location? The axillary region (armpit area). But accessory breasts have been documented in unusual locations, including the back, thigh, and even the vulvar region.
Medical case reports document a 15-year-old boy with two accessory nipples—one in the forearm and one along the standard milk line. This demonstrates how developmental variations can occur outside typical patterns.
Symptoms and When Treatment Becomes Necessary
Many people with polymastia remain asymptomatic throughout their lives. The condition often resembles a mole or skin tag and causes no problems.
But here’s where it gets interesting. About one-third of women presenting with accessory breast tissue experience symptoms during menstruation or lactation. Hormonal stimulation during puberty, pregnancy, and breastfeeding can activate dormant breast tissue.
Symptoms include:
- Swelling and tenderness during menstrual cycles
- Milk production from accessory tissue during lactation
- Pain or discomfort in the affected area
- Cosmetic concerns
- Potential for developing breast disease, including cancer
According to NIH research, accessory breast tissue carries the same disease risks as normal breast tissue. Malignancy can develop in ectopic breast tissue, making monitoring important.
The Truth About Surgical Third Breasts
Beyond natural polymastia, surgical creation of a third breast has gained attention through viral stories. According to online reports, a woman claimed to have spent $20,000 on a procedure to add a third breast, though the authenticity of this surgical claim remains disputed among medical professionals.
Dr. Kevin Tehrani, a plastic surgeon, publicly stated he didn’t believe the procedure actually occurred. Real talk: creating a functional third breast surgically presents significant medical and ethical challenges.
Plastic surgeons can relocate tissue and create breast-like structures, but engineering a fully functional mammary gland from scratch isn’t standard practice. Most documented cases of “three breasts” involve naturally occurring polymastia, not surgical creation.
Diagnosis and Treatment Options
Diagnosis of polymastia typically occurs during physical examination. Most supernumerary breast tissue can be identified during standard chest and abdominal examinations because of its distribution along the milk line.
For confirmation, imaging studies may include:
- Ultrasound to visualize tissue structure
- Mammography for larger masses
- MRI in complex cases
- Histological examination after removal
Treatment depends on symptoms and patient preference. Asymptomatic accessory breast tissue doesn’t require intervention. Many people live their entire lives unaware they have the condition.
When Surgery Makes Sense
Surgical removal becomes appropriate when:
- Tissue causes pain or discomfort
- Cosmetic concerns affect quality of life
- Tissue undergoes suspicious changes
- Lactation from accessory tissue creates problems
- Patient requests removal for personal reasons
The surgical procedure involves excision of the ectopic breast tissue. According to medical literature, this is performed as prophylaxis against potential malignancy and for aesthetic reasons.
Recovery is typically straightforward, with most patients resuming normal activities within weeks.
Familial Patterns and Genetic Factors
Medical literature documents familial polythelia occurring across multiple generations in some families. This suggests genetic components influence breast development anomalies.
Polymastia may appear with familial polythelia even without renal anomalies, though associations with congenital anomalies are well documented. Medical evaluations sometimes include screening for kidney and urological issues when supernumerary breast tissue is identified.
The atavistic nature of polythelia—its connection to evolutionary traits seen in mammals with multiple breast pairs—has been studied extensively. This developmental variation represents an incomplete regression of features common in other mammalian species.
| Condition | Definition | Prevalence | Typical Location |
|---|---|---|---|
| Polymastia | Extra breast tissue with/without nipple | 0.22-6% | Along milk line, often axillary |
| Polythelia | Extra nipples without breast tissue | 2-5% | Milk line from axilla to groin |
| Complete accessory breast | Full breast with nipple and areola | Rare subset | Usually axillary region |
| Intraareolar polythelia | Extra nipple within existing areola | Extremely rare | Within normal breast areola |
Frequently Asked Questions
While three complete breasts with full nipple-areola complexes and functional glandular tissue is extremely rare, polymastia can produce this outcome. Most cases involve partial breast tissue development rather than three identical breasts.
Supernumerary nipples (polythelia) are less common in women than in men. However, symptomatic polymastia with significant glandular tissue tends to be diagnosed more frequently in women due to hormonal activation during puberty, menstruation, and pregnancy.
Yes. Fully functional ectopic breast tissue can lactate during pregnancy and breastfeeding. About one-third of women with accessory breast tissue experience symptoms during lactation, including milk production from the supernumerary tissue.
Accessory breast tissue carries the same disease risks as normal breast tissue, including the potential for developing breast cancer. Any suspicious changes in supernumerary breast tissue warrant medical evaluation.
Polythelia refers specifically to extra nipples, typically without associated breast tissue. Polymastia indicates the presence of actual glandular breast tissue, which may or may not include a nipple and areola.
While most cases occur along the embryonic milk line from axilla to groin, rare case reports document accessory breast tissue in unusual locations including the back, shoulder, thigh, and vulvar region.
Removal depends on individual circumstances. Asymptomatic tissue often requires no treatment. Surgery is recommended when tissue causes pain, cosmetic concerns, undergoes suspicious changes, or interferes with normal activities.
Living With Supernumerary Breast Tissue
For most people with polymastia, the condition requires no medical intervention. The tissue remains dormant and causes no symptoms.
But wait. Hormonal changes can activate previously dormant tissue. Women may notice swelling, tenderness, or even milk production during pregnancy and lactation. Understanding this possibility helps manage expectations.
Regular monitoring makes sense, especially for larger areas of ectopic breast tissue. The same screening recommendations that apply to normal breast tissue—self-examination, clinical evaluation, and appropriate imaging—extend to accessory breasts.
Cosmetic concerns vary widely. Some people feel self-conscious about visible accessory tissue, while others consider it an interesting anatomical variation. There’s no right or wrong response—personal preference drives treatment decisions.
The Bottom Line on Three Breasts
So, is it possible to have three breasts? Absolutely. Medical science confirms that polymastia allows for the development of supernumerary breast tissue, creating what could be considered a third breast.
The condition isn’t as rare as commonly believed, affecting up to 6% of the population in some regions. Most presentations involve accessory nipples or small patches of breast tissue rather than fully formed additional breasts.
Natural polymastia represents a developmental variation along the embryonic milk line. While viral stories of surgical third breast creation capture attention, most documented cases involve this congenital condition rather than cosmetic procedures.
Understanding polymastia helps demystify this anatomical variation. For those affected, awareness of symptoms, monitoring recommendations, and treatment options enables informed healthcare decisions.
If concerns arise about unusual tissue along the chest, abdomen, or axillary regions, consult a healthcare provider. Proper diagnosis ensures appropriate management and peace of mind.