
Quick Summary: Blocking sperm from coming out—either voluntarily or due to medical conditions like retrograde ejaculation—is generally not harmful to physical health. The body naturally reabsorbs unused sperm without negative side effects. However, sperm blockage can affect fertility and may cause discomfort in some cases, require medical evaluation if conception is desired or symptoms persist.
The question of what happens when sperm is blocked from coming out concerns many people. Some deliberately hold back ejaculation based on ancient beliefs about semen conservation, while others experience involuntary blockage due to medical conditions.
Understanding the mechanisms behind sperm blockage helps separate myth from medical reality. The nervous system controls both erection and ejaculation through complex pathways involving the sympathetic and parasympathetic systems.
This article examines the medical facts about blocking sperm, the body’s natural response, potential health implications, and when medical attention becomes necessary.
Understanding Normal Ejaculation Process
Before exploring what happens when sperm is blocked, it’s important to understand normal ejaculatory function. According to research published in Translational Andrology and Urology, ejaculation involves coordinated nervous system activity.
The parasympathetic nervous system maintains relaxed physiological states, while the sympathetic system activates during sexual climax. At ejaculation, heart rate can increase by 100% due to sympathetic effects, as documented in Biology journal research from 2022.
Normal ejaculation occurs in distinct stages. The emission phase involves secretions from the seminal vesicles contribute 65-75% of the ejaculate volume, the prostate contributes roughly 25-30%, vasal fluid supplies 5-10%. These fluids mix to form semen.
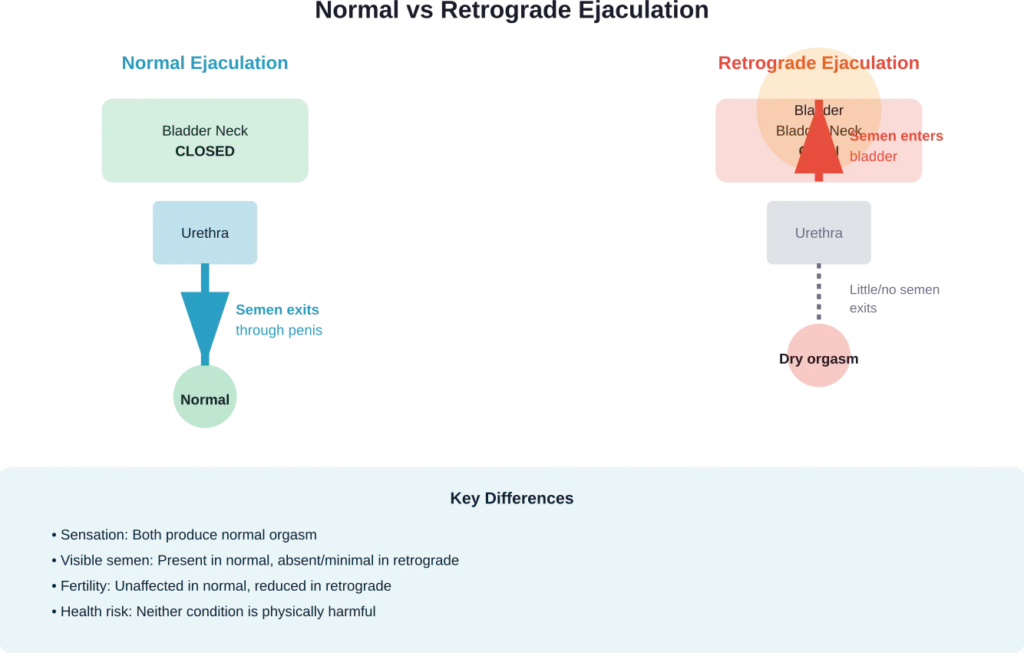
During the expulsion phase, rhythmic contractions propel semen through the urethra and out through the penis. A small circular muscle called the bladder neck sphincter closes during this process, preventing semen from entering the bladder.
This coordinated sequence depends on intact nerve pathways and properly functioning muscles. Disruption at any point can alter where sperm goes when ejaculation occurs.
What Is Retrograde Ejaculation?
Retrograde ejaculation represents the most common form of involuntary sperm blockage. This condition occurs when semen enters the bladder instead of exiting through the penis during orgasm.
The bladder neck sphincter normally closes during ejaculation, directing semen forward. When this muscle fails to contract properly, semen takes the path of least resistance backward into the bladder.
Men with retrograde ejaculation still experience orgasm and sexual pleasure. The key difference is little or no visible semen emerges from the penis—sometimes called a “dry orgasm.”
According to medical research on ejaculatory physiology, retrograde ejaculation has several potential causes:
- Surgical damage to bladder muscles or controlling nerves (prostate surgery, bladder neck surgery)
- Diabetes-related nerve damage
- Medications that affect muscle tone, particularly alpha-blockers like tamsulosin
- Spinal cord injuries affecting nerve signals
- Multiple sclerosis or other neurological conditions
Research on tamsulosin published in medical journals shows this medication can cause ejaculatory changes, though it may not negatively impact overall sexual function compared to placebo.
What Happens to Blocked Sperm in the Body?
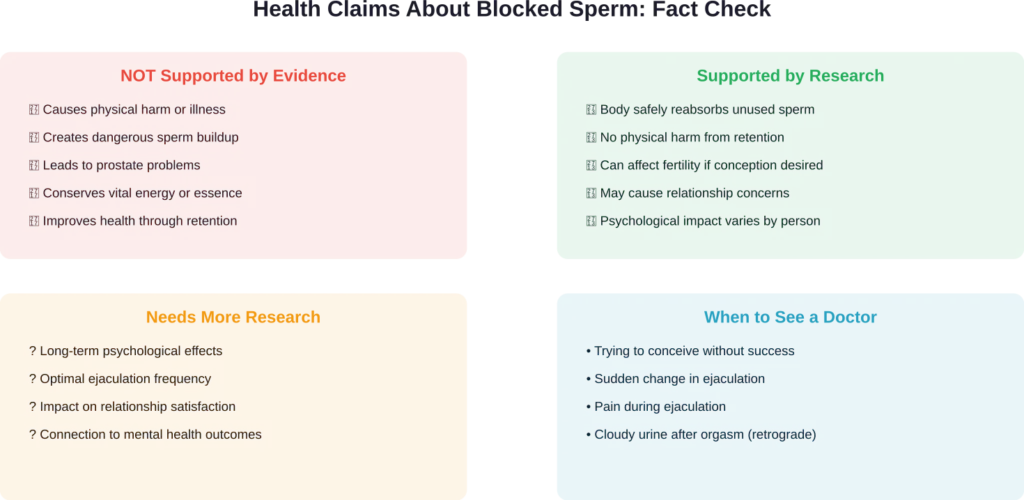
Here’s the important part: when sperm cannot exit the body, it doesn’t cause harm. The body has natural mechanisms to handle unused sperm.
Medical research confirms that sperm and semen that don’t leave the body are simply reabsorbed. In cases of retrograde ejaculation, semen enters the bladder and exits later during urination.
For men who voluntarily abstain from ejaculation or experience other forms of blockage, sperm that remains in the reproductive tract breaks down naturally. The body recycles the cellular components without negative effects.
According to data from research on ejaculation frequency and health published in Frontiers in Psychology, there’s no evidence that retaining sperm causes physical harm. The body continuously produces new sperm—approximately 1,500 per second in healthy males.
The testicular environment naturally manages sperm production and disposal. Old sperm cells undergo a process called apoptosis (programmed cell death) and are broken down by specialized cells.
Does Sperm Build Up Create Pressure or Pain?
Some men worry that not ejaculating will cause painful sperm buildup. Generally speaking, this isn’t a medical concern for most people.
The body regulates sperm production based on storage capacity. When the epididymis (sperm storage structure) reaches capacity, production slows and older sperm are reabsorbed.
That said, some men report temporary discomfort from prolonged sexual arousal without release—sometimes called “blue balls” (epididymal hypertension). This discomfort typically resolves on its own within hours and isn’t caused by sperm accumulation but by sustained blood flow to the genital area.
Voluntary Semen Retention: Ancient Practice Meets Modern Medicine
Some people deliberately practice semen retention based on traditional beliefs that conserving semen improves health, energy, or vitality. Ancient Chinese medicine considered semen more valuable than blood, according to historical medical texts.
Modern research provides a more nuanced picture. Studies examining ejaculation frequency and health outcomes show mixed results depending on what’s measured.
Research published in peer-reviewed journals suggests that frequent ejaculation may reduce prostate cancer risk. The proposed mechanisms include:
- Suppression of sympathetic nervous system activity
- Regular flushing of potentially carcinogenic substances from the prostate
- Changes in gene expression in prostate tissue
- Reduced cellular division rates in prostate epithelial cells
However, research on ejaculation frequency and mental health shows that regular sexual activity—including masturbation—correlates with various wellness indicators. Research data indicates 61% of men in an American sample reported masturbatory behavior over the past year.
The takeaway? Current evidence doesn’t support health benefits from deliberately blocking or withholding ejaculation. Conversely, there’s no evidence it causes harm either.
Medical Conditions That Block Sperm
Beyond retrograde ejaculation, several medical conditions can prevent sperm from exiting normally. Understanding these helps identify when medical evaluation is needed.
| Condition | Mechanism | Primary Impact |
|---|---|---|
| Anejaculation | Complete absence of ejaculation despite orgasm | Fertility issues, requires medical evaluation |
| Delayed Ejaculation | Marked delay or infrequency of ejaculation | Sexual frustration, relationship strain |
| Urethral Stricture | Narrowing of urethra blocks semen passage | Ejaculatory pain, reduced flow |
| Obstruction (vas deferens) | Physical blockage prevents sperm transport | Infertility, normal ejaculate but no sperm |
| Medication-induced | Drugs affecting nerve or muscle function | Variable effects on ejaculation |
Research on ejaculatory disorders in men with urethral stricture indicates that improvement in ejaculation after surgical correction occurs primarily in younger men.
Medications represent a common reversible cause. According to published medical research, drugs affecting alpha-1 adrenergic receptors frequently cause ejaculatory dysfunction. Examples include certain blood pressure medications, antidepressants, and antipsychotic drugs.
When Physical Blockage Requires Treatment
Physical obstructions in the reproductive tract differ from functional issues like retrograde ejaculation. Vas deferens obstruction can result from:
- Vasectomy (intentional sterilization)
- Infection-related scarring
- Congenital absence
- Surgical complications
According to the American College of Obstetricians and Gynecologists, vasectomy intentionally blocks sperm transport as permanent contraception. After vasectomy, sexual function doesn’t change—sperm normally make only 5 percent of semen.
The remaining 95% of ejaculate comes from the prostate and seminal vesicles, so there’s little change in fluid volume released during orgasm.
Health Effects: Separating Fact From Fiction
Now for the evidence-based answer to whether blocking sperm causes health problems. Current medical research indicates blocking sperm from coming out is not harmful to physical health.
Research from the National Institutes of Health examining ejaculatory dysfunction and its impact finds that the primary concerns are fertility-related and psychological rather than physical health threats.
Let’s look at what the research does and doesn’t support:
Fertility Implications
The primary medical concern with blocked sperm is fertility. Men trying to conceive need sperm to reach the egg, which requires normal antegrade (forward-moving) ejaculation.
Retrograde ejaculation doesn’t make a man sterile—sperm are still produced and can be retrieved from urine samples for assisted reproduction techniques. However, natural conception becomes extremely difficult.
According to research on ejaculatory physiology and male infertility, various treatments can help. For retrograde ejaculation caused by medications, stopping or switching drugs may restore normal function. For nerve-related causes, medications like pseudoephedrine (an alpha agonist) can sometimes help close the bladder neck sphincter.
Research on pseudoephedrine efficacy exists in the medical literature, though treatment protocols may vary by clinical context.
Psychological and Relationship Effects
While physically safe, sperm blockage can create psychological distress. Research published in Translational Andrology and Urology emphasizes that ejaculatory function exists within a dyadic (two-person) process.
Both partners’ perceptions of the condition impact relationship satisfaction. Men may feel concerned about:
- Reduced visible evidence of orgasm
- Concerns about masculinity or sexual function
- Anxiety about fertility
- Partner’s perception of sexual satisfaction
According to studies examining ejaculatory dysfunction’s impact on couples, communication and understanding between partners significantly affects how the condition influences relationship quality.
Common Misconceptions About Ejaculation
Several myths persist about holding back ejaculation. Let’s address the most common ones.
Myth 1: Semen contains vital life force that should be conserved. While traditional medicine systems held this belief, modern biology shows semen is a combination of fluids and cells that the body produces continuously. No evidence supports vitality loss from ejaculation.
Myth 2: Not ejaculating increases testosterone. Scientific literature indicates complex relationships between testosterone and sexual function; claims about sustained testosterone elevation from abstaining should be discussed with healthcare providers.
Myth 3: Frequent ejaculation causes weakness or fatigue. Current research suggests regular ejaculation does not cause physical weakness or energy depletion.
Myth 4: Holding back ejaculation improves sexual performance. While techniques to delay ejaculation can help manage premature ejaculation, completely blocking ejaculation doesn’t improve sexual function. Premature ejaculation is characterized as the ‘most common male sexual dysfunction,’ with a prevalence rate of 20–30% according to research using DSM-IV-TR definitions.
Treatment Options for Involuntary Blockage
When sperm blockage occurs involuntarily and causes concern—particularly for fertility—several treatment approaches exist.
| Treatment Type | Best For | Success Rate Notes |
|---|---|---|
| Medication adjustment | Drug-induced retrograde ejaculation | Often reversible by stopping or switching medications |
| Alpha-agonist drugs | Retrograde ejaculation from nerve issues | Variable effectiveness; pseudoephedrine most studied |
| Sperm retrieval | Fertility concerns with persistent blockage | Allows assisted reproduction techniques |
| Surgical correction | Structural abnormalities or strictures | Depends on specific condition and age |
| Behavioral techniques | Delayed ejaculation | May help when psychological factors present |
The choice of treatment depends on the underlying cause and whether fertility is a concern. For men not seeking to conceive, many forms of ejaculatory dysfunction require no treatment if sexual satisfaction remains intact.
When to Seek Medical Evaluation
Most cases of blocked sperm don’t require emergency care. However, medical evaluation makes sense in certain situations.
Consider seeing a healthcare provider if:
- Sudden changes in ejaculation pattern occur
- Attempting conception without success for 6-12 months
- Pain accompanies ejaculation
- Cloudy urine consistently appears after orgasm (suggests retrograde ejaculation)
- Complete absence of ejaculation with orgasm develops
- Ejaculatory changes follow new medication or surgery
A urologist or sexual medicine specialist can perform appropriate diagnostic tests. For retrograde ejaculation, medical tests such as post-orgasm urine analysis can help confirm diagnosis.
Additional testing might include hormone panels, neurological assessment, or imaging studies depending on suspected causes.
The Bottom Line on Blocked Sperm
So what really happens if you block sperm from coming out? The evidence-based answer is reassuring: it’s not harmful to physical health.
The body has natural mechanisms to handle sperm that don’t exit through ejaculation. Whether through reabsorption in the reproductive tract or passage into the bladder and later urination, unused sperm are safely managed without health consequences.
The primary concerns with blocked sperm relate to fertility and psychological well-being rather than physical danger. For couples trying to conceive, sperm blockage obviously presents a challenge that may require medical intervention.
Ancient beliefs about semen conservation lack support from modern medical research. Neither withholding ejaculation nor experiencing blockage provides health benefits. Conversely, regular ejaculation appears safe and may even offer some protective effects against certain conditions.
The key is understanding your specific situation. Deliberate semen retention as a personal or spiritual practice is safe if that’s your choice. Involuntary blockage that concerns you—especially regarding fertility—warrants medical evaluation to identify causes and explore solutions.
Real talk: your body is designed to manage sperm production and disposal efficiently. Trust the process and seek help when changes in function concern you or affect your goals.
Frequently Asked Questions
No, deliberately holding back ejaculation is not physically harmful. The body will naturally reabsorb unused sperm without negative health effects. Some people practice this for personal or cultural reasons. However, there’s no evidence that sperm retention provides health benefits either. If this practice causes discomfort or relationship issues, it may be worth reconsidering.
Treatment success for retrograde ejaculation depends on the cause. Medication-induced cases often improve when drugs are stopped or changed. Nerve damage from diabetes or surgery may be harder to reverse, though medications like pseudoephedrine can help in some cases. Sperm can be retrieved from urine for fertility purposes even when retrograde ejaculation persists. Consult a urologist for evaluation and treatment options specific to your situation.
Short-term abstinence of 2-5 days can increase sperm concentration in ejaculate, which is why fertility testing often recommends this timeframe. However, abstinence beyond about a week doesn’t continue to increase sperm count and may actually reduce sperm quality. The body continuously produces sperm and maintains balance between production and reabsorption. For fertility purposes, moderate ejaculation frequency appears optimal rather than prolonged retention.
Sudden onset of dry orgasm (little or no semen during ejaculation) can result from several causes: starting new medications (especially blood pressure or prostate drugs), recent surgery involving the bladder or prostate, development of diabetes-related nerve issues, or urinary tract infection. This represents a form of retrograde ejaculation or anejaculation and warrants medical evaluation, especially if it appeared suddenly or concerns you.
True sperm blockage typically doesn’t cause pain or swelling. The body reabsorbs sperm that can’t exit. However, some men experience temporary discomfort from prolonged arousal without release, sometimes called epididymal hypertension. This usually resolves within hours. Persistent pain, testicular swelling, or discomfort during ejaculation suggests other issues like infection, injury, or structural problems and requires medical evaluation.
Most men with retrograde ejaculation report normal orgasms and sexual pleasure. The sensation of orgasm doesn’t depend on semen exiting through the penis—it’s primarily a neurological response. Some men initially feel concerned about the lack of visible ejaculate, which can create psychological distress. However, the physical pleasure of orgasm typically remains intact. Communication with partners about the condition helps maintain sexual satisfaction.
Sperm don’t accumulate indefinitely when blocked. In the epididymis (storage area), sperm can remain viable for several weeks. However, the body continuously produces new sperm while breaking down and reabsorbing older ones. There’s no dangerous buildup—the reproductive system maintains balance through natural processes. Whether sperm exit through ejaculation or are reabsorbed internally, the body manages the process safely without timeframe concern