Quick Summary: Accidentally injecting a small amount of air into muscle tissue is generally harmless. The air gets absorbed by the body within 24-48 hours without causing significant problems. However, large volumes of air entering the bloodstream can cause a serious condition called air embolism, though this requires substantial amounts and is extremely rare with intramuscular injections.
The sight of air bubbles in a syringe can trigger instant panic. But does that tiny bubble spell disaster?
Here’s the thing—context matters enormously. The muscle versus vein distinction, the amount of air involved, and the injection technique all determine whether you’re dealing with a non-event or a medical emergency.
Most concerns about air injection stem from confusion between intramuscular and intravenous administration. They’re fundamentally different scenarios with vastly different risk profiles.
Understanding Air in Intramuscular Injections
Intramuscular injections place medication deep into muscle tissue. According to StatPearls, bulky muscles have good vascularity, allowing injected drugs to quickly reach systemic circulation while bypassing first-pass metabolism.
When small air bubbles enter muscle tissue, they don’t cause harm. The air simply gets absorbed.
Community discussions among healthcare workers confirm that small amounts of air (0.2cc–0.3cc) in manufacturer-filled syringes don’t need to be expelled before intramuscular injection. This amount won’t cause tissue damage or systemic complications.
The muscle tissue acts as a buffer. Unlike direct venous access, air introduced into muscle doesn’t immediately enter the bloodstream in dangerous quantities.
What About the Air-Lock Technique?
Interestingly, some injection protocols deliberately use air. Research published in Saudi Medical Journal examined the air-lock technique (ALT) for intramuscular injections.
This technique involves drawing a small air bubble into the syringe after medication. The air follows the medication into the muscle, creating a “lock” that prevents medication from leaking back along the needle track.
The study found mean pain scores after injections using this technique ranged from 2.53 to 3.30 on a visual analog scale—demonstrating the technique’s safety and tolerability.
When Air Becomes Dangerous: Air Embolism Explained
Air embolism occurs when gas bubbles enter the vascular system and block blood flow. This is where things get serious.
But here’s what matters: the volume required to cause problems is substantial.
According to StatPearls, venous gas embolism (VGE) represents the abnormal accumulation of gas forming bubbles within the systemic venous circulation. These bubbles act as emboli and disrupt blood flow.
Most VGE cases are iatrogenic—caused by medical procedures. Approximately 90% of reported cases occur during central venous cannulation, head and neck surgery, or other invasive procedures.
Intramuscular vs. Intravenous: The Critical Difference
The route of administration dramatically changes risk profiles.
Intravenous injections place substances directly into veins. Air introduced this way enters circulation immediately. Central venous catheters and pressurized intravenous infusion systems pose the highest risk.
Intramuscular injections deliver medication into muscle tissue. Air must diffuse from muscle into capillaries—a much slower process involving smaller quantities.
Real talk: the scenarios that cause fatal air embolism involve continuous air sources or large-bore venous access. A single small bubble in an intramuscular injection doesn’t create these conditions.
Clinical Presentation of Air Embolism
When air embolism does occur, symptoms depend on the volume and location of trapped air.
According to research published in Diagnostics, air embolism cases showed varying severity. Many cases remained clinically silent and unreported, while symptomatic VGE required immediate intervention due to potential cardiovascular collapse.
| Severity Level | Volume Range | Typical Symptoms |
|---|---|---|
| Asymptomatic | Small amounts | No clinical signs, body absorbs air naturally |
| Mild to Moderate | Variable | Chest discomfort, shortness of breath, cough |
| Severe | Large volumes | Cardiovascular collapse, altered consciousness, seizures |
A study examining 67 air embolism cases found that 94% occurred in-hospital, with 77.8% happening during an operation or invasive procedure. Vascular access-related procedures accounted for 33% of cases.
Sound familiar? That’s because the highest-risk scenarios involve surgical settings, not routine intramuscular medications.
Treatment and Management
If significant air embolism occurs, treatment focuses on preventing further air entry and supporting cardiovascular function.
According to the Cleveland Clinic, treatment may include:
- 100% high-flow oxygen through a nasal cannula or hyperbaric chamber
- Positioning the body to prevent air from traveling to vital organs
- Maintaining airway patency and blood pressure
- Supportive care tailored to the embolism’s location
Hyperbaric oxygen therapy compresses gas bubbles, making them smaller and easier for the body to absorb. This treatment proves particularly valuable for arterial gas embolism.
But wait—this level of intervention applies to serious cases. Minor air exposure from intramuscular injections won’t trigger these protocols.
Prevention and Safe Injection Practices
The CDC emphasizes safe injection practices as every provider’s responsibility. According to CDC guidelines, a safe injection doesn’t harm the patient, expose the provider to risks, or result in hazardous waste.
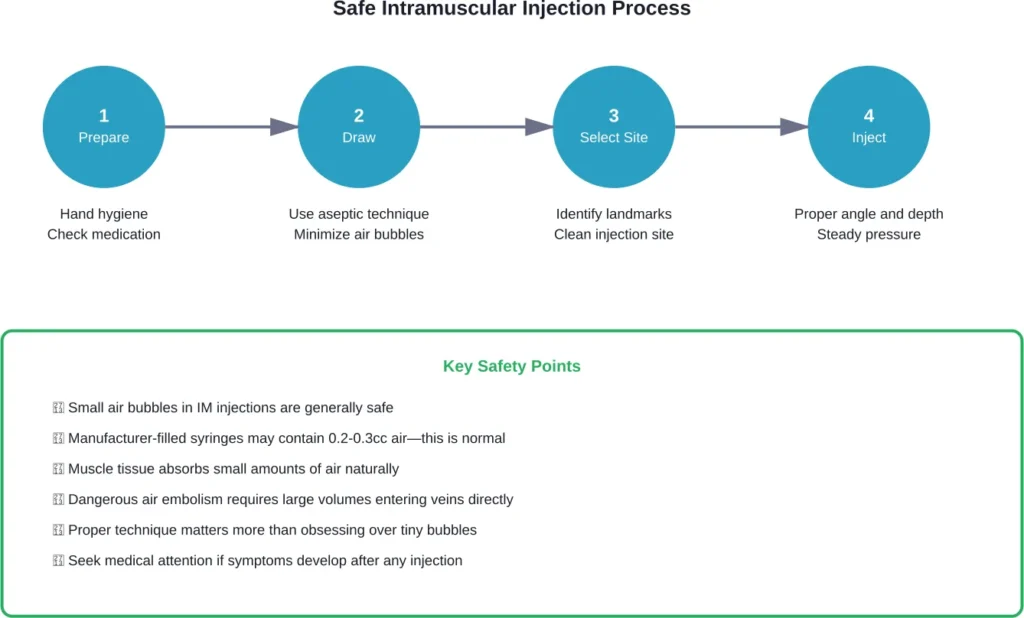
Healthcare workers should follow these principles:
- Cleanse hands with alcohol-based antiseptic or soap and water before preparing vaccines
- Use aseptic technique throughout injection preparation
- Follow manufacturer guidelines for medication preparation
- Inspect syringes for defects or contamination
The CDC also notes that for non-live vaccines, manufacturers typically recommend use within the same day that a vaccine is withdrawn or reconstituted.
What About Home Injections?
Many patients administer intramuscular or subcutaneous injections at home. Common concerns arise about air bubbles in self-filled syringes.
Healthcare guidance suggests tapping the syringe to move bubbles to the top, then gently pushing the plunger to expel large bubbles. However, obsessing over every microscopic bubble isn’t necessary.
The priority is proper injection technique—correct site selection, appropriate needle angle, and steady medication delivery.
Rare Complications Worth Knowing
While small air volumes in intramuscular injections are safe, certain medical contexts deserve mention.
Research documented cases of oxygen embolism caused by accidental subcutaneous injection of hydrogen peroxide during orthopedic surgery. This involved specialized circumstances—not routine medication administration.
An estimated 57% of orthopedic surgeries produce detectable air embolisms, though most remain clinically insignificant. The surgical context involves open tissue planes and direct vascular exposure—entirely different from closed intramuscular injection.
During endoscopic retrograde cholangiopancreatography (ERCP), research indicates a 2.4% incidence for venous air embolism. This reflects the procedure’s invasive nature and pressurized air use.
These examples underscore that context determines risk. Simple intramuscular medication delivery doesn’t create the conditions necessary for dangerous air embolism.
Frequently Asked Questions
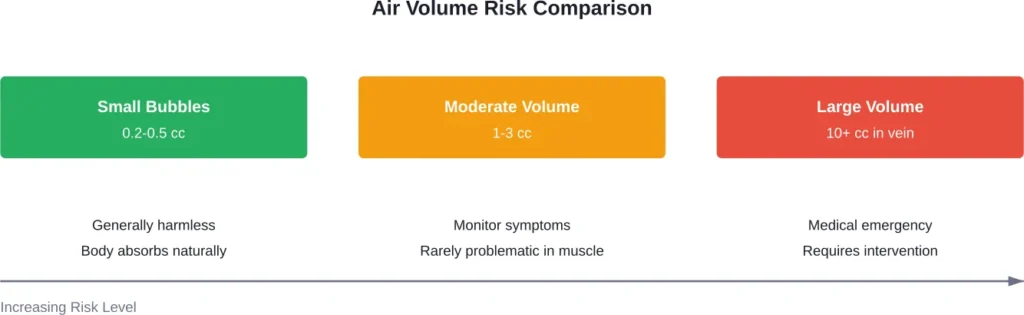
No. Small air bubbles (0.2-0.5cc) in intramuscular injections won’t cause harm. The muscle tissue absorbs the air naturally within 24-48 hours. Dangerous air embolism requires much larger volumes entering veins directly, not muscle tissue.
Research indicates lethal air embolism requires substantial volumes of air entering the venous system rapidly. Even smaller amounts (10-20cc) can cause symptoms if introduced quickly into central circulation. Intramuscular injections don’t create these conditions with typical small air bubbles.
Symptoms vary by severity and location. Mild cases may cause chest discomfort or shortness of breath. Severe cases can produce altered consciousness, cardiovascular collapse, or seizures. Most intramuscular injections with small air bubbles produce no symptoms whatsoever.
For small amounts from a typical syringe, emergency care isn’t necessary. Monitor for unusual symptoms like severe chest pain, difficulty breathing, or altered consciousness. If you injected a large volume (multiple cc) or develop concerning symptoms, seek medical evaluation.
Manufacturer-filled vaccine syringes may contain 0.2-0.3cc of air intentionally. This small amount doesn’t need to be expelled before injection. Some protocols use the air-lock technique, where air follows medication to prevent leakage along the needle track.
Intramuscular injections place air into muscle tissue, where it gets absorbed slowly and safely. Intravenous injections put air directly into veins, where it can enter circulation immediately. The intravenous route poses significantly higher risk, though even then, small bubbles are typically harmless.
Small amounts of air injected into muscle tissue typically absorb within 24-48 hours. The body’s natural processes dissolve and eliminate the air through surrounding tissue without intervention or complications.
Final Thoughts
The fear of air bubbles in injections often exceeds the actual risk—especially for intramuscular administration.
Medical research consistently demonstrates that small air volumes in muscle injections are harmless. The body naturally processes them. Dangerous air embolism requires specific conditions: large volumes, direct venous access, and rapid introduction.
Proper injection technique, sterile practices, and appropriate site selection matter far more than obsessing over microscopic bubbles.
If administering medications at home, focus on following your healthcare provider’s instructions. Minimize air when drawing medication, but don’t let anxiety about tiny bubbles prevent taking necessary medications.
When in doubt, consult your healthcare provider. They can address specific concerns about medication, injection technique, and individual risk factors. Safe injection practices protect your health—but understanding the actual risks helps with confident injection rather than fearful administration.