
Quick Summary: Touching dry ice causes immediate cold burns (frostbite) because it sits at -109°F (-78°C), freezing skin cells on contact. Even brief exposure creates tissue damage that resembles heat burns, with potential for blistering, numbness, and permanent scarring depending on duration.
Dry ice looks deceptively harmless. It’s just solid carbon dioxide, right? But here’s the thing—this innocent-looking block sits at a bone-chilling -109°F (-78°C), cold enough to cause serious tissue damage within seconds.
Direct contact with dry ice triggers what medical professionals call a cold burn or frostbite injury. The extreme temperature freezes skin cells instantly, creating damage that’s remarkably similar to burns from heat sources.
Community discussions reveal just how easy it is to underestimate this hazard. People report holding dry ice through plastic bags for mere moments and ending up with painful blisters that take weeks to heal.
Understanding What Dry Ice Really Is
Dry ice is solid carbon dioxide, fundamentally different from the frozen water cubes sitting in your freezer. While regular ice melts into liquid, dry ice sublimates—it transforms directly from solid to gas without any liquid phase.
This sublimation happens at -109°F (-78°C), according to the University of Illinois Division of Research Safety. That’s substantially colder than water ice at 32°F (0°C). The temperature difference matters enormously for skin safety.
One pound of dry ice produces 250 liters of carbon dioxide gas. Within 24 hours, 5-10 pounds can sublimate completely, potentially creating oxygen displacement hazards in enclosed spaces.
The Immediate Physical Response to Contact
When skin touches dry ice, cellular freezing begins immediately. The extreme cold causes ice crystals to form within and between cells, damaging cell membranes and disrupting tissue structure.
Blood vessels constrict rapidly in response to the cold, reducing circulation to the affected area. This vasoconstriction—while a natural protective mechanism—actually compounds the injury by limiting oxygen and nutrient delivery to already-damaged tissue.
The sensation during contact often surprises people. Instead of feeling cold, many report a burning sensation. This happens because the same nerve pathways process both extreme cold and heat signals, creating what’s sometimes called a “paradoxical heat sensation.”
Stages of Cold Burn Severity
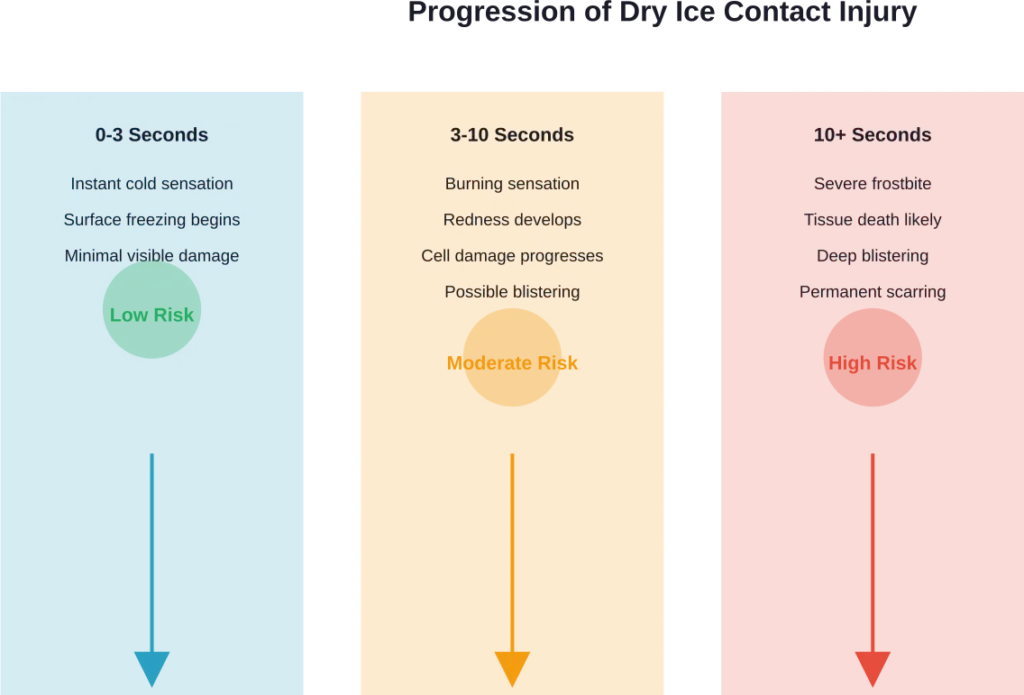
Not all dry ice burns are equal. The severity depends primarily on contact duration and whether moisture was present (wet skin freezes faster than dry).
First-Degree Cold Burns
Brief contact—less than three seconds—typically produces first-degree burns. The outer skin layer becomes red and painful, similar to mild sunburn. These heal within days without scarring.
Second-Degree Cold Burns
Contact lasting several seconds creates second-degree burns. Blisters form as fluid accumulates between skin layers. The affected area becomes numb initially, then transitions to intense pain as sensation returns. Healing takes weeks, and scarring becomes possible.
Third-Degree Cold Burns
Prolonged contact causes third-degree burns, affecting all skin layers and potentially underlying tissue. The area may appear white, waxy, or blackened. Nerve damage creates numbness that can persist permanently.
| Burn Degree | Contact Duration | Symptoms | Healing Time |
|---|---|---|---|
| First-Degree | Under 3 seconds | Redness, mild pain | 3-7 days |
| Second-Degree | 3-10 seconds | Blistering, intense pain | 2-3 weeks |
| Third-Degree | Over 10 seconds | Tissue death, numbness | Weeks to months |
First Aid Treatment Protocol
Quick action after dry ice contact significantly impacts recovery outcomes. Cleveland Clinic recommends specific steps for treating cold burns effectively.
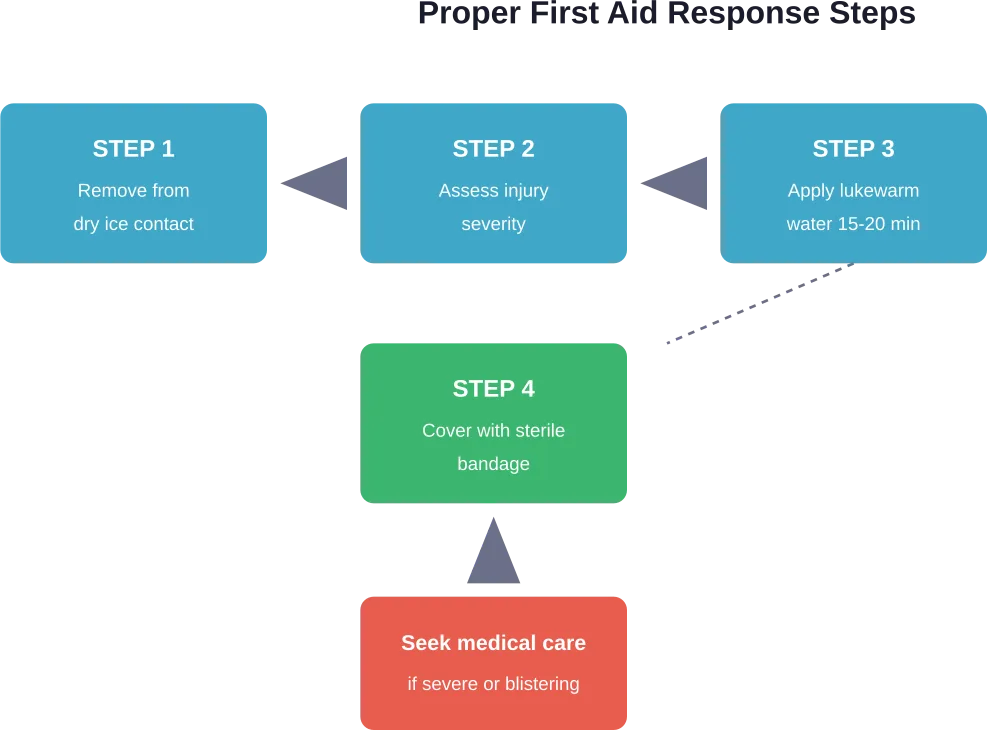
Start by moving away from the dry ice source immediately. Don’t attempt to rub or massage the affected area—this can cause additional tissue damage.
Warm the area gradually using lukewarm water (not hot) for 15 to 20 minutes. Temperature matters here. Water that’s too hot creates thermal shock, potentially worsening tissue damage. Aim for water around 98-102°F (37-39°C).
Moist heat works well as an alternative. A heating pad on low setting provides gentle, controlled warming.
Never use direct heat sources like hair dryers, heating pads on high, or open flames. The damaged tissue can’t properly sense temperature, making it vulnerable to additional burns.
When Medical Attention Becomes Necessary
Most minor dry ice burns can be treated at home, but certain situations require professional medical evaluation. Seek immediate care if blisters larger than a quarter form, if the affected area becomes white or grayish, or if numbness persists beyond initial rewarming.
According to research published in the National Library of Medicine, cold-induced injuries that penetrate beyond superficial skin layers need professional assessment. Deep tissue damage isn’t always immediately apparent.
Children and individuals with conditions affecting circulation—like diabetes or peripheral vascular disease—should receive medical evaluation even for seemingly minor cold burns. These populations face higher complication risks.
Safe Handling Practices That Actually Work
Protection during dry ice handling isn’t optional—it’s essential. Insulated gloves specifically rated for cryogenic temperatures provide adequate protection. Regular winter gloves won’t suffice; they’re not designed for extreme cold exposure.
Cornell University’s Environment, Health and Safety department emphasizes using appropriate tools like tongs or scoops rather than relying solely on protective gloves. This creates distance between hands and the ice surface.
Work in well-ventilated areas always. Remember that sublimation produces substantial carbon dioxide gas. Concentrations of more than 0.5% (5000 ppm) carbon dioxide in the air can lead to unconsciousness, according to the University of Illinois Division of Research Safety.
Transport dry ice in containers that allow gas escape. Never seal it in airtight containers or standard coolers without ventilation—pressure buildup can cause container rupture.
Common Misconceptions About Dry Ice Safety
Several dangerous myths persist about dry ice handling. Let’s address them directly.
Myth: Touching dry ice briefly won’t cause harm. Reality: Damage begins within seconds. Even momentary contact can cause first-degree burns.
Myth: Wet gloves provide adequate protection. Reality: Moisture accelerates freezing. Wet fabric conducts cold more effectively than dry material, increasing injury risk.
Myth: Dry ice stored in a freezer lasts longer. Reality: Freezers aren’t cold enough to prevent sublimation. Dry ice will sublimate regardless of freezer storage, potentially building dangerous pressure in enclosed freezer compartments.
Long-Term Effects and Complications
Severe cold burns can produce lasting consequences beyond initial healing. Nerve damage from deep frostbite may cause permanent numbness or altered sensation in affected areas.
Research on cold-induced injuries indicates that cold-induced injuries can create lasting changes in temperature sensitivity. Previously injured areas often become more susceptible to future cold damage.
Scarring from second and third-degree cold burns can be significant. Tissue that’s frozen and damaged deeply may not regenerate with normal skin architecture, leaving visible and textural changes.
FAQs
There’s no truly safe duration for bare skin contact with dry ice. Even one to two seconds can cause first-degree burns. Always use proper insulated gloves or tools when handling dry ice to prevent any direct contact.
Most people report a burning sensation rather than cold when touching dry ice. This happens because extreme cold and heat activate the same pain receptors, creating what’s called paradoxical heat sensation. The injury is still from freezing despite the hot feeling.
Regular gloves won’t provide adequate protection. Only insulated gloves specifically rated for cryogenic temperatures effectively prevent cold burns from dry ice. Standard winter gloves or cotton work gloves allow the extreme cold to penetrate within seconds.
Remove contact immediately and warm the affected area gradually with lukewarm water for 15-20 minutes. Avoid hot water, rubbing the area, or using direct heat sources. Cover with a sterile bandage and seek medical attention if blistering or severe pain develops.
Seek medical care if blisters form, the skin turns white or grayish, numbness persists after rewarming, or the affected area is larger than three inches. Third-degree cold burns may appear waxy or blackened and require immediate professional treatment.
First-degree burns typically heal without scarring. Second-degree burns may leave discoloration or minor scarring. Third-degree cold burns often produce permanent scars and may cause lasting nerve damage with altered sensation in the affected area.
Never allow dry ice to contact your mouth, lips, or internal tissues. While small amounts can create visual effects in beverages, the ice must fully sublimate before consumption. Direct ingestion causes severe internal cold burns to mouth, throat, and digestive tissue.
Understanding the Real Risk
Dry ice demands respect. That -109°F temperature isn’t just a number—it’s cold enough to cause permanent tissue damage faster than most people realize.
The key takeaway? Never handle dry ice with bare hands, regardless of how brief you think the contact will be. Proper protective equipment isn’t excessive caution; it’s basic safety protocol backed by decades of occupational health research.
If contact does occur, treat it seriously. Follow proper first aid protocols, monitor for complications, and don’t hesitate to seek medical evaluation for anything beyond minor redness.
Handle dry ice safely, respect its extreme temperature, and you’ll avoid joining the countless people who’ve learned this lesson the painful way.