
Quick Summary: Having too much potassium (hyperkalemia) occurs when blood potassium levels exceed 5.5 mEq/L, typically due to kidney disease, certain medications, or excessive intake. While mild cases may cause no symptoms, severe hyperkalemia can trigger life-threatening cardiac arrhythmias, muscle weakness, and paralysis. Treatment ranges from dietary modifications and medication adjustments to emergency interventions like dialysis, depending on severity and underlying cause.
Potassium keeps muscles working, nerves firing, and the heart beating properly. But there’s a dangerous flip side to this essential mineral.
When potassium levels climb too high in the bloodstream, the body enters a state medical professionals call hyperkalemia. According to StatPearls (NIH), hyperkalemia is defined as a serum or plasma potassium concentration exceeding the upper normal limit, typically greater than 5.0 to 5.5 mEq/L.
Here’s what makes this condition particularly tricky: mild elevations often produce zero symptoms. Yet severe cases can trigger cardiac arrest within hours.
Understanding Hyperkalemia: When Good Potassium Goes Bad
Potassium is an electrolyte that regulates fluid balance, muscle contractions, and nerve signals throughout the body. The American Heart Association notes that maintaining proper potassium levels is critical for heart function.
In healthy individuals, hyperkalemia remains relatively uncommon. Medical experts estimate that 2% to 3% of the general population experiences high potassium levels. But the risk multiplies for people with chronic kidney disease—they’re up to three times more likely to develop this condition.
The kidneys normally act as potassium gatekeepers, filtering excess amounts from the blood. According to research published by the NIH, renal adaptive mechanisms allow kidneys to maintain potassium homeostasis until the glomerular filtration rate drops below 15 ml/min/1.73 m².
When this system fails, potassium accumulates.
Symptoms: From Silent to Life-Threatening
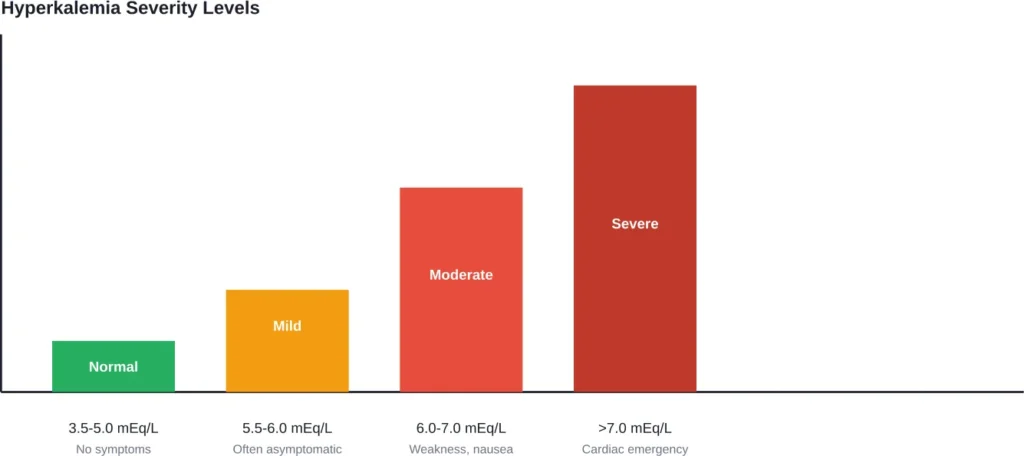
Mild hyperkalemia operates like a stealth problem. Many people experience no symptoms whatsoever when potassium levels hover between 5.5 and 6.0 mEq/L.
Symptoms usually develop at higher levels, 6.5 mEq/L to 7 mEq/L, though the rate of change is more important than the absolute potassium level.
Someone whose potassium spikes suddenly may develop severe symptoms at lower levels. Meanwhile, patients with chronic hyperkalemia from kidney impairment may tolerate higher concentrations without obvious signs.
Common Warning Signs Include:
- Muscle weakness or fatigue
- Numbness or tingling sensations
- Nausea and vomiting
- Difficulty breathing
- Chest pain or palpitations
- Slow or irregular heartbeat
The most dangerous symptom? Cardiac arrhythmias. High potassium interferes with electrical signals that coordinate heartbeats, potentially causing fatal rhythm disturbances.
What Causes Potassium Levels to Spike?
Hyperkalemia results from three primary mechanisms: reduced renal excretion, excessive intake, or leakage from cells into the bloodstream.
Kidney Disease
This represents the leading cause. According to medical research, approximately 10% of the daily potassium intake is cleared via the gastrointestinal tract, with kidneys filtering the remainder. When kidney function deteriorates, this filtration system fails.
Chronic kidney disease patients face the highest risk, particularly once glomerular filtration rate drops significantly.
Medications
Certain drugs interfere with potassium regulation. According to medical research, drug-induced hyperkalemia is extremely common. The combination of ACE inhibitors and spironolactone, for instance, frequently triggers elevated potassium levels.
Common medication culprits include:
- ACE inhibitors and ARBs (blood pressure medications)
- Potassium-sparing diuretics
- NSAIDs (pain relievers)
- Certain antibiotics
- Immunosuppressants
Dietary Factors
While rare in healthy individuals, excessive potassium intake can overwhelm the kidneys. High-potassium foods include bananas, oranges, potatoes, spinach, avocados, and beans.
Approximately 10% of daily potassium intake is cleared through the gastrointestinal tract. When kidneys fail, this proportion increases—but not enough to prevent accumulation.
Other Medical Conditions
Hyperkalemia may result from acute volume depletion due to dehydration, hemorrhage, or reduced effective circulating blood volume associated with congestive heart failure or cirrhosis, according to NIH research.
Tubular dysfunction, aldosterone deficiency, tissue breakdown, and metabolic acidosis can also trigger potassium release from cells.
Diagnosis: How Doctors Detect High Potassium
Blood tests provide the definitive diagnosis. A basic metabolic panel measures serum potassium concentration.
But doctors don’t stop there. Since hyperkalemia affects the heart’s electrical system, an electrocardiogram (ECG) becomes essential for evaluating cardiac risk.
ECG changes progress as potassium rises: peaked T waves appear first, followed by widened QRS complexes, and eventually sine wave patterns indicating imminent cardiac arrest.
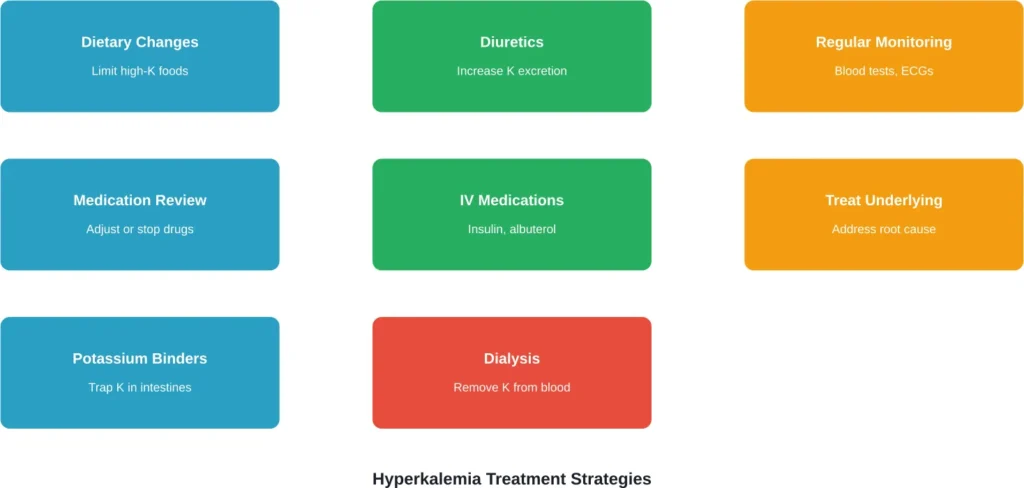
Treatment Options: From Diet to Dialysis
Treatment intensity scales with severity. Mild cases may require only medication adjustments and dietary changes. Severe hyperkalemia demands immediate emergency intervention.
| Severity Level | Potassium Range | Treatment Approach |
|---|---|---|
| Mild | 5.5-6.0 mEq/L | Diet modification, medication review |
| Moderate | 6.0-7.0 mEq/L | Oral potassium binders, diuretics |
| Severe | >7.0 mEq/L | IV calcium, insulin/glucose, dialysis |
Emergency Interventions
According to research on treatment of hyperkalemic emergencies published in World Journal of Emergency Medicine, acute treatment focuses on three goals: stabilizing cardiac membranes, shifting potassium into cells, and removing excess potassium from the body.
Calcium gluconate or calcium chloride protects the heart without lowering potassium levels. Insulin with glucose drives potassium back into cells temporarily. Dialysis physically removes potassium from the bloodstream.
Long-Term Management
For chronic hyperkalemia, doctors typically prescribe:
- Potassium binders (medications that trap potassium in the intestines)
- Dietary restrictions limiting high-potassium foods
- Medication adjustments to avoid drugs that raise potassium
- Regular monitoring through blood tests
The National Kidney Foundation emphasizes working with a kidney dietitian to create safe eating plans, particularly for patients following plant-based diets who may struggle with potassium restrictions.
Who’s at Highest Risk?
Certain populations face elevated risk for developing too much potassium:
- Chronic kidney disease patients (especially stages 3-5)
- People taking multiple blood pressure medications
- Diabetics, particularly with kidney complications
- Elderly individuals with declining kidney function
- Heart failure patients on specific medication regimens
- Those with Addison’s disease or other endocrine disorders
Infants naturally maintain higher baseline potassium levels than children and adults, according to NIH research.
Prevention: Keeping Potassium in Check
For people at risk, prevention focuses on vigilance rather than avoidance. Potassium remains essential for health—the goal is maintaining balance.
Key prevention strategies include:
- Regular blood tests to monitor potassium levels
- Working with healthcare providers to review medications
- Following dietary recommendations from kidney specialists
- Staying hydrated to support kidney function
- Avoiding potassium supplements unless prescribed
- Reading food labels for potassium content
The CDC notes that sodium and potassium work together as electrolytes to maintain fluid and blood volume. Too much sodium and too little potassium can raise blood pressure—but the inverse creates different problems.
Balance matters more than absolute avoidance.
The Bottom Line on Too Much Potassium
Hyperkalemia operates on a spectrum from harmless to deadly. While healthy kidneys typically prevent dangerous accumulation, kidney disease, medications, and certain medical conditions can tip the scales.
The asymptomatic nature of mild hyperkalemia makes regular monitoring essential for at-risk populations. When symptoms do appear—particularly cardiac irregularities—immediate medical attention becomes critical.
Treatment works, but prevention remains ideal. Anyone with kidney disease or taking multiple medications should maintain regular contact with healthcare providers and monitor potassium levels through routine blood work.
The American Heart Association emphasizes that mild cases are usually easy to treat when caught early. Severe cases require emergency intervention but respond well to appropriate therapy.
If diagnosed with hyperkalemia, working closely with doctors and following treatment recommendations can prevent progression to life-threatening complications. Potassium management is achievable—it just requires attention and appropriate medical guidance.
Frequently Asked Questions
No, drinking water doesn’t directly cause hyperkalemia. However, severe overhydration can dilute blood sodium levels, which may indirectly affect electrolyte balance. High potassium typically results from kidney dysfunction, medications, or excessive dietary intake rather than fluid consumption alone.
Limit bananas, oranges, potatoes, spinach, tomatoes, avocados, dried fruits, beans, nuts, and dairy products. Also avoid salt substitutes, which often contain potassium chloride. The National Kidney Foundation recommends working with a dietitian to create a personalized low-potassium eating plan that maintains proper nutrition.
Emergency treatments can lower potassium within minutes to hours. Calcium stabilizes the heart within 1-3 minutes, insulin shifts potassium into cells within 15-30 minutes, and dialysis removes potassium over 2-4 hours. Long-term management through diet and medication adjustments produces gradual changes over days to weeks.
Hyperkalemia itself is reversible with proper treatment. However, the underlying cause may be chronic. People with advanced kidney disease often require ongoing management to prevent recurrence. Those with medication-induced hyperkalemia typically resolve completely after drug adjustments, assuming normal kidney function.
Intense exercise can temporarily shift potassium from muscle cells into the bloodstream, causing transient elevation. However, healthy kidneys quickly restore normal levels. Stress alone doesn’t directly raise potassium, though stress-related dehydration may affect electrolyte balance. These temporary fluctuations differ from true hyperkalemia.
Healthy individuals can consume potassium-rich foods without developing hyperkalemia because functioning kidneys efficiently excrete excess amounts. Hyperkalemia occurs when kidney disease, medications, or metabolic problems prevent proper potassium elimination. The World Health Organization recommends potassium-rich diets for most healthy adults despite high intake.
Testing frequency depends on risk factors and severity. People with stable chronic kidney disease typically require monitoring every 3-6 months. Those starting new medications that affect potassium may need checks within 1-2 weeks, then monthly until stable. High-risk patients or those with previous hyperkalemia episodes require more frequent surveillance—doctors determine appropriate schedules individually.