Quick Summary: High cholesterol causes plaque buildup in arteries, significantly increasing the risk of heart attack and stroke. According to the CDC, millions of Americans have this condition, which often shows no symptoms until serious cardiovascular events occur. The good news: lifestyle changes and medication can effectively lower cholesterol levels and reduce these risks.
Cholesterol gets a bad reputation, but here’s the thing: your body actually needs it. According to the CDC, blood cholesterol is a waxy, fat-like substance made by your liver, and it’s essential for good health. Your body uses it to make hormones and digest fatty foods.
But when cholesterol levels climb too high, it becomes a silent threat lurking in your bloodstream.
Millions of people in the United States have high cholesterol. Most don’t even know it because this condition rarely announces itself with obvious symptoms. Instead, it quietly damages arteries over months and years, setting the stage for potentially life-threatening cardiovascular events.
Understanding What Cholesterol Actually Does
The CDC emphasizes that your liver makes all the blood cholesterol your body needs. Cholesterol travels through blood on proteins called lipoproteins, and there are two main types that matter for your health.
LDL (low-density lipoprotein) cholesterol earned its nickname as “bad” cholesterol for good reason. It makes up most of your body’s cholesterol, and high levels of LDL cholesterol raise your risk for heart disease and stroke. This is the type that can accumulate in artery walls.
HDL (high-density lipoprotein) cholesterol is the “good” kind. It actually helps remove other forms of cholesterol from your bloodstream, carrying them back to your liver for disposal.
Research from the National Institutes of Health shows that serum total cholesterol and LDL-C levels are associated with increased cardiovascular disease mortality, while HDL-C levels are inversely associated with cardiovascular death. Translation? High LDL hurts you, high HDL helps you.
The Silent Damage High Cholesterol Causes
High cholesterol doesn’t hurt. It doesn’t make you tired. It doesn’t cause headaches or nausea.
That’s precisely what makes it dangerous.
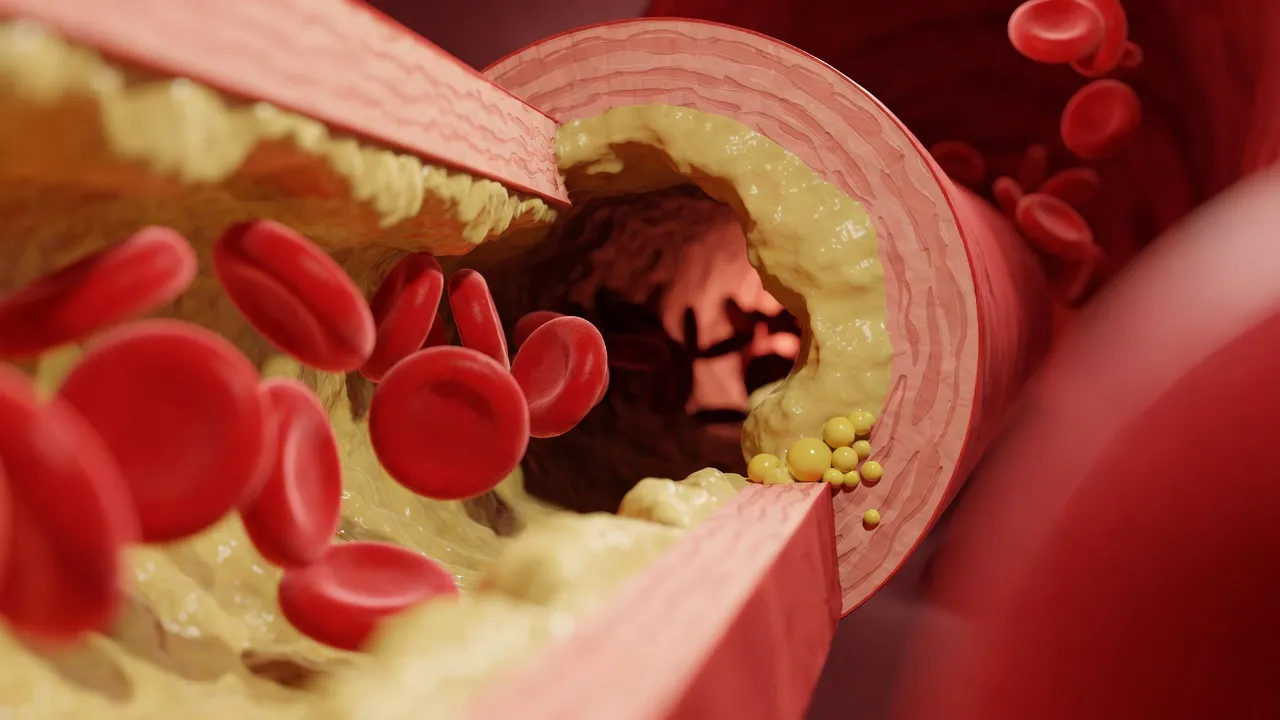
According to the CDC, optimal total blood cholesterol is less than 150 mg/dL. When levels exceed this, fats and other substances can build up in blood vessels called arteries. This buildup is called plaque.
How Plaque Destroys Your Arteries
As more plaque forms over time, arteries become narrowed or clogged. This process—called atherosclerosis—happens gradually and silently. The plaque deposits contain cholesterol, fatty substances, cellular waste products, calcium, and fibrin.
Think of it like mineral deposits building up in old water pipes. The flow gets restricted, pressure increases, and eventually something has to give.
But here’s where it gets worse. Plaque doesn’t just narrow arteries—it can rupture. When plaque breaks open, blood cells called platelets rush to the site to try to repair the damage. This creates blood clots that can completely block blood flow.
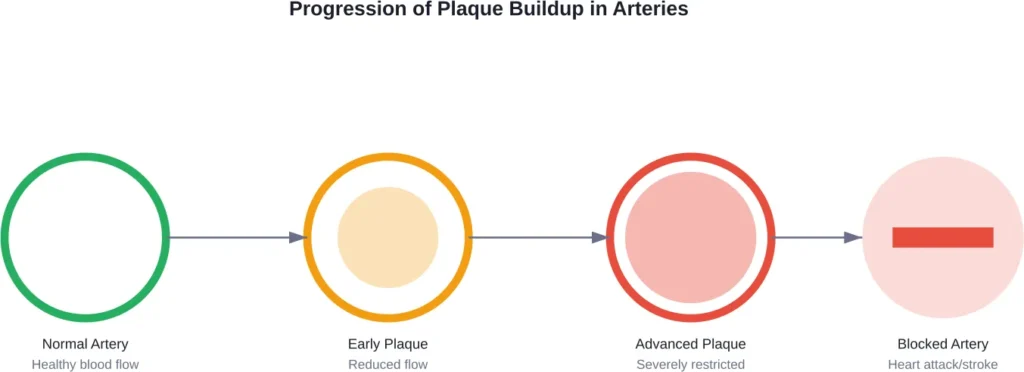
Heart Attack and Stroke: The Ultimate Consequences
When arteries that supply blood to your heart become severely narrowed or blocked, you get a heart attack. When the same happens to arteries feeding your brain, you get a stroke.
According to the CDC, high cholesterol is one of the key risk factors for heart disease. Research published in medical journals shows that for every mmol/L (approximately 39 mg/dL) reduction in LDL cholesterol with statin therapy, there is an approximate 22% reduction in ASCVD events.
That’s not a small difference. That’s the gap between life and death for many people.
A meta-analysis of seven studies comprising 506,813 patients (118,491 statin users and 388,322 non-users), with a mean follow-up of 3.7 years, found that statin therapy significantly reduced all-cause mortality (relative risk 0.60, 95% CI: 0.43-0.83) and MACE (relative risk 0.75, 95% CI: 0.70-0.82).
Beyond Heart Attack and Stroke
High cholesterol doesn’t limit its damage to your heart and brain. Peripheral artery disease—where plaque builds up in arteries supplying blood to your legs and feet—is another serious consequence.
Research shows that elevated remnant cholesterol increases the risk of peripheral artery disease.
Why High Cholesterol Shows No Symptoms
Here’s what makes high cholesterol particularly insidious: it causes no symptoms until something catastrophic happens.
You won’t feel plaque accumulating in your arteries. You won’t notice your blood vessels narrowing. Most people feel completely fine right up until they have a heart attack or stroke.
The only way to know if you have high cholesterol is through a blood test. This measures total cholesterol, HDL cholesterol, LDL cholesterol, and triglycerides—another type of fat in your blood.
Health professionals may ask patients to fast for 8 to 12 hours before the test, drinking only water. This gives the most accurate reading of cholesterol levels.
Who’s Most at Risk
According to the CDC, certain factors increase the risk for high cholesterol. Some can’t be controlled, like age and family history. But others are entirely within reach to change.
| Uncontrollable Risk Factors | Controllable Risk Factors |
|---|---|
| Age (risk increases after 50) | Diet high in saturated fats |
| Family history of high cholesterol | Lack of physical activity |
| Familial hypercholesterolemia (genetic disorder) | Being overweight or obese |
| Being male or post-menopausal | Smoking |
| South Asian or sub-Saharan African origin | Excessive alcohol consumption |
Familial hypercholesterolemia is a classical genetic disorder caused by mutations in the LDL-receptor gene. This results in LDL cholesterol greater than 190 mg/dL in heterozygotes and greater than 450 mg/dL in homozygotes. This defect in the LDL receptor accounts for at least 85% of familial hypercholesterolemia cases.
But for most people, lifestyle choices play the dominant role.
The Diabetes and Chronic Kidney Disease Connection
People with diabetes or chronic kidney disease face even higher risks. Research shows that being above both LDL-C and non-HDL-C thresholds was associated with increased rates of cardiovascular outcomes—particularly pronounced in those with diabetes or chronic kidney disease.
Being above both LDL-C and non-HDL-C thresholds was associated with a hazard ratio of 1.16 for those with diabetes or chronic kidney disease (HR: 1.16; 95% CI: 1.09-1.23) and 1.10 for people without these conditions (HR: 1.10; 95% CI: 1.05-1.15).
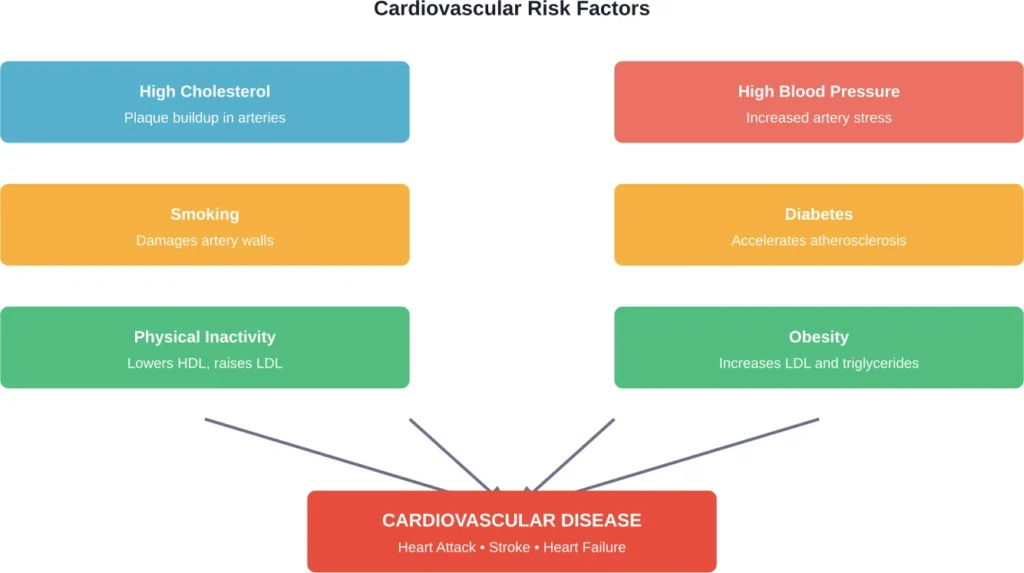
The Combined Threat: Cholesterol Plus Blood Pressure
High cholesterol rarely works alone. When combined with high blood pressure, the risk multiplies dramatically.
Research has shown that combined high systolic blood pressure and elevated serum cholesterol significantly increase cardiovascular disease risk. This combination effect was far worse than either condition alone.
According to the CDC, several health conditions combine to increase heart disease risk, with high blood pressure and high cholesterol leading the list.
What Your Cholesterol Numbers Actually Mean
Not all cholesterol levels carry the same risk. Understanding what the numbers mean helps put things in perspective.
| Cholesterol Type | Optimal Level | Borderline High | High Risk |
|---|---|---|---|
| Total Cholesterol | Less than 200 mg/dL | 200-239 mg/dL | 240 mg/dL and above |
| LDL Cholesterol | Less than 100 mg/dL | 130-159 mg/dL | 160 mg/dL and above |
| HDL Cholesterol | 60 mg/dL and above | 40-59 mg/dL | Less than 40 mg/dL |
| Triglycerides | Less than 150 mg/dL | 150-199 mg/dL | 200 mg/dL and above |
According to CDC guidance, total blood cholesterol should be kept as low as possible, with less than 200 mg/dL generally considered desirable. But context matters—someone with multiple other risk factors might need lower targets than someone who’s otherwise healthy.
Very high triglyceride levels (over 1000 mg/dL) carry increased health risks.
How to Lower Your Cholesterol
The good news? High cholesterol responds well to treatment. Both lifestyle changes and medication can bring levels down and reduce cardiovascular risk.
Lifestyle Changes That Actually Work
According to health authorities, lifestyle modifications form the foundation of cholesterol management. Lifestyle modifications can help lower LDL cholesterol levels.
Exercise matters significantly. Health guidelines recommend that adults aged 18-64 years should aim for 30 to 60 minutes of moderate-intensity physical activity on most days of the week. For those 65 years and older, 30 minutes total of moderate-intensity physical activity daily is recommended.
Both aerobic exercises and resistance training help improve cholesterol profiles. Regular physical activity raises HDL (good) cholesterol while lowering LDL (bad) cholesterol and triglycerides.
Dietary changes make a substantial difference too. Reducing saturated fats—found in red meat, full-fat dairy products, and tropical oils—directly impacts LDL levels. Your liver makes all the cholesterol your body needs, so dietary cholesterol from animal-based foods just adds to the load.
Smoking cessation is critical. Smoking damages artery walls, making them more susceptible to plaque accumulation. It also lowers HDL cholesterol.
Alcohol moderation helps as well. Drinking less—or not at all—can improve cholesterol numbers and reduce overall cardiovascular risk.
When Medication Becomes Necessary
For many people, lifestyle changes alone aren’t enough. That’s where medication enters the picture.
Statins are the most widely used cholesterol-lowering drugs. Research shows impressive results: for every mmol/L (approximately 39 mg/dL) reduction in LDL cholesterol with statin therapy, there is an approximate 22% reduction in ASCVD events.
Other medications include ezetimibe, which blocks cholesterol absorption in the intestines, and PCSK9 inhibitors, which help the liver remove more LDL cholesterol from the blood. Bempedoic acid is a newer option that reduces cholesterol production in the liver.
Guidelines from the American Heart Association, American College of Cardiology, and European organizations emphasize several key principles: the sooner treatment starts, the greater the benefit; the greater the decrease in LDL-C, the greater the benefit; the higher the LDL-C level, the greater the benefit; and the higher the absolute risk of cardiovascular disease, the greater the benefit.
The Long-Term Outlook
High cholesterol is manageable, but it requires ongoing attention. Left untreated, it will continue damaging arteries year after year.
Research on treat-to-target cholesterol-lowering interventions shows that achieving and maintaining target levels significantly reduces cardiovascular disease and all-cause mortality risk. Studies with 29-year follow-up periods demonstrate that the benefits accumulate over time.
Recent cohort studies show that meeting both LDL-C and non-HDL-C thresholds after starting statin therapy leads to better outcomes. Those who achieved both targets had significantly lower rates of cardiovascular events during follow-up periods averaging 2.5 years.
But here’s the reality: high cholesterol is typically a lifelong condition. Even when medication brings numbers down to optimal ranges, stopping treatment usually causes levels to climb back up.
Special Populations and Considerations
Different groups face unique challenges with cholesterol management.
Women’s risk changes dramatically after menopause. The hormonal shifts that occur can raise LDL cholesterol and lower HDL cholesterol, increasing cardiovascular risk. Women who’ve been through menopause should be particularly vigilant about cholesterol monitoring.
People of South Asian or sub-Saharan African origin face higher baseline risks and may develop high cholesterol at younger ages. These populations often benefit from earlier screening and more aggressive treatment targets.
Age matters too. Risk increases steadily as people get older, with those over 50 facing substantially higher odds of developing high cholesterol and experiencing cardiovascular events.
Prevention: Starting Before Problems Begin
The CDC emphasizes that by living a healthy lifestyle, it’s possible to keep cholesterol in a healthy range and lower the risk of heart disease and stroke.
Prevention works best when it starts early. Children of parents with high cholesterol or heart disease should have their levels checked. Building healthy habits in youth—regular exercise, nutritious eating, avoiding smoking—pays dividends for decades.
Regular cholesterol screening is recommended. Those with risk factors may need more frequent testing.
Frequently Asked Questions
No, high cholesterol causes no symptoms. Most people feel completely normal until a serious event like heart attack or stroke occurs. The only way to detect high cholesterol is through a blood test. This is why it’s often called a “silent” condition—it damages arteries for years without any warning signs.
The timeline varies significantly. Plaque buildup typically occurs over many years or even decades. However, once substantial plaque exists, a rupture can trigger a heart attack within minutes. Some people develop dangerous plaque in their 30s and 40s, while others maintain healthier arteries into old age. This depends on cholesterol levels, other risk factors, genetics, and lifestyle choices.
Total cholesterol above 240 mg/dL is considered high risk. LDL cholesterol above 160 mg/dL also indicates high risk. But context matters—someone with diabetes or previous heart attack may need much lower targets. People with familial hypercholesterolemia can have LDL levels exceeding 190 mg/dL or even 450 mg/dL, which require aggressive treatment.
For some people, yes. Significant lifestyle changes—diet modifications, regular exercise, weight loss, smoking cessation—can lower LDL cholesterol. But many people, particularly those with genetic predispositions or very high levels, need medication to reach safe targets. The decision depends on individual cholesterol levels, overall cardiovascular risk, and response to lifestyle interventions.
High cholesterol doesn’t directly cause leg pain, but peripheral artery disease resulting from cholesterol buildup can. When plaque narrows arteries supplying blood to the legs, it causes pain during walking (called claudication). Research shows elevated remnant cholesterol carries increased risk of peripheral artery disease. The pain typically occurs in the calves, thighs, or buttocks during exercise and subsides with rest.
Statins are effective at lowering cholesterol, with healthcare providers typically checking levels after an initial period to assess effectiveness. Healthcare providers usually check cholesterol levels after this period to assess whether the medication is working effectively and whether dosage adjustments are needed. Statins work by blocking an enzyme the liver uses to produce cholesterol.
Absolutely. Your liver makes most of your blood cholesterol—diet contributes, but genetics often plays the larger role. People with familial hypercholesterolemia have genetic mutations affecting how their bodies process cholesterol, leading to high levels regardless of diet. Even with excellent eating habits, some people need medication to control cholesterol. That said, diet still matters significantly and can help lower levels alongside medication.
Taking Control of Your Cholesterol
High cholesterol sets in motion a cascade of events that damages arteries and dramatically increases the risk of heart attack, stroke, and peripheral artery disease. Plaque accumulates silently, year after year, causing no symptoms until something catastrophic happens.
But it doesn’t have to end that way.
Regular screening catches high cholesterol before it causes irreversible damage. Lifestyle changes—improved diet, regular exercise, smoking cessation, weight management—can significantly lower levels and reduce risk. When needed, medications like statins provide powerful additional protection, with research showing substantial reductions in cardiovascular events and mortality.
The key is action. Waiting for symptoms means waiting too long. Get your cholesterol checked, understand your numbers, and work with healthcare providers to develop a treatment plan that addresses your specific risk factors.
According to the CDC and other health authorities, managing cholesterol is one of the most effective ways to prevent heart disease and stroke. The evidence is clear, the tools are available, and the benefits are substantial. What happens with high cholesterol depends entirely on whether action is taken—or whether the silence continues until arteries can no longer deliver the blood your heart and brain need to survive.