Quick Summary: When a person with an implantable cardioverter defibrillator (ICD) dies, the device may continue delivering shocks even during the final moments of life. Nearly 30% of ICD patients receive shocks at end-of-life, which don’t meaningfully extend survival but can cause distress for patients and families. Most ICD recipients actually die from heart failure or non-cardiac causes rather than sudden cardiac arrest, making end-of-life planning and potential device deactivation important conversations to have with healthcare providers.
Implantable cardioverter defibrillators save countless lives by detecting dangerous heart rhythms and delivering corrective shocks. But here’s what many patients don’t realize: these devices don’t distinguish between a life-threatening arrhythmia that occurs during otherwise good health and one that happens during the natural dying process.
This creates a complex situation that deserves honest discussion. The same device designed to protect you can, in certain circumstances, interfere with a peaceful death.
How ICDs Function During the Dying Process
An implantable cardioverter defibrillator continuously monitors heart rhythm. When it detects ventricular tachycardia or ventricular fibrillation, it responds automatically—either with pacing, a lower-energy cardioversion, or a full shock.
The device doesn’t know whether you’re experiencing a sudden, potentially reversible cardiac event or entering the final stages of terminal illness. It simply does what it’s programmed to do: try to restore normal rhythm.
During the natural dying process, irregular heart rhythms frequently occur. These arrhythmias are often part of the body’s natural shutdown. When an ICD is still active, it interprets these rhythms as threats and delivers shocks accordingly.
Research shows that nearly 30% of patients with defibrillators receive shocks at the end of life. These shocks don’t meaningfully prolong survival but can cause significant distress.
What Patients and Families Experience
ICD shocks are painful. Patients often describe them as being kicked in the chest by a horse. Imagine experiencing this sensation repeatedly during your final hours or days.
For family members present during this time, witnessing these shocks can be traumatic. The physical jolt is visible—the body literally jumps with each discharge. This can transform what should be a peaceful goodbye into a distressing medical event.
Some patients remain conscious during end-of-life shocks, experiencing both the physical pain and the emotional awareness of what’s happening. Others may be unconscious, but families still witness the device firing.
How Most ICD Patients Actually Die
Here’s a fact that surprises many people: most ICD recipients don’t die from sudden cardiac arrest.
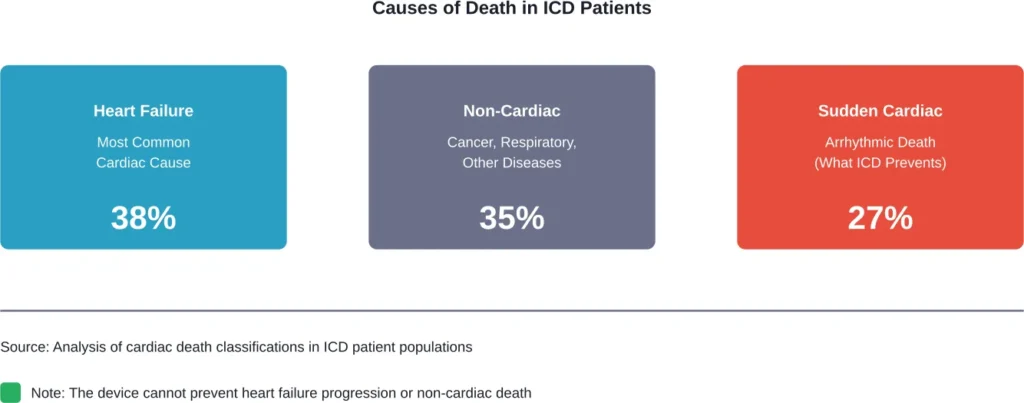
According to research analyzing patients with implantable defibrillators or cardiac resynchronization therapy devices with defibrillator capability, the majority die from heart failure or non-cardiac causes rather than the sudden arrhythmic death the device was meant to prevent.
When researchers examined causes of death among ICD patients, they found heart failure was the most common cardiac cause. Non-cardiac causes—including cancer, respiratory disease, and other conditions—also accounted for a significant portion of deaths.
This matters because it challenges a common assumption. Many patients believe their ICD will prevent their death indefinitely. In reality, while the device effectively prevents sudden cardiac death from arrhythmias, it doesn’t address the underlying progression of heart disease or other life-limiting conditions.
Understanding ICD Deactivation Options
Patients and families have the right to request ICD deactivation. This is a medical decision, not euthanasia or suicide.
Turning off the shock function doesn’t kill you. It simply allows natural processes to occur without technological interference. The device can still provide pacing support for bradycardia (slow heart rate) even when the defibrillation function is deactivated.
This distinction matters. Many patients worry that deactivating their ICD means giving up or hastening death. In reality, deactivation becomes relevant primarily when someone is already dying from their underlying condition or another terminal illness.
When Patients Consider Deactivation
Several situations prompt conversations about ICD deactivation:
- Terminal cancer diagnosis or other life-limiting non-cardiac illness
- Advanced heart failure that’s no longer responding to treatment
- Entering hospice or palliative care
- Multiple device infections requiring removal without replacement
- Personal preference after careful consideration of goals
Current guidelines actually recommend against ICD placement in patients with life expectancy less than one year. But many patients receive their devices when prognosis is better, then face changing circumstances years later.
According to research on one-year mortality after ICD placement, identifying patients who might benefit from early palliative care conversations remains challenging. Disease trajectories change, and what made sense at implantation may need reconsideration later.
The Communication Gap
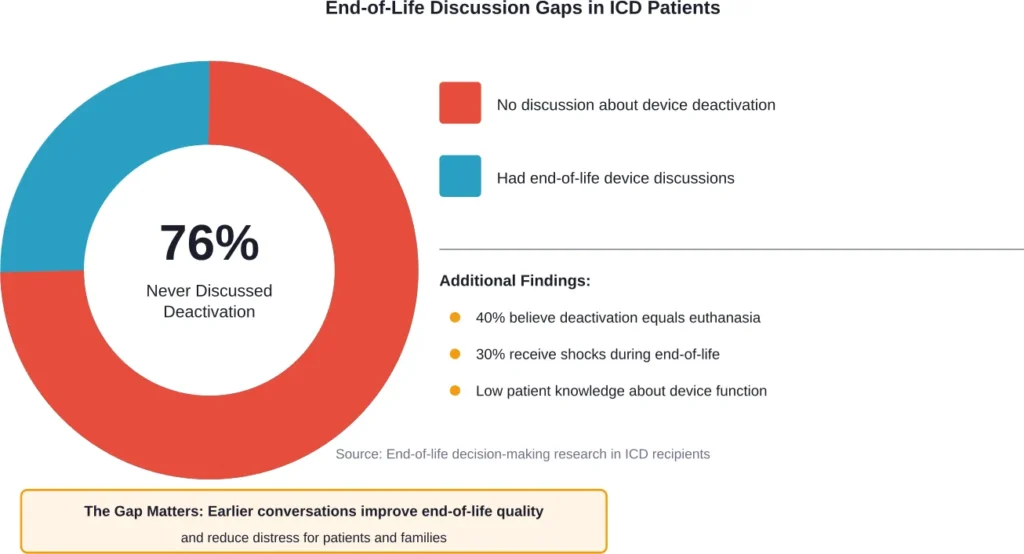
Here’s a troubling statistic: research shows that 76% of ICD patients report never discussing the implications of future device deactivation with their healthcare provider.
That’s not a typo. Three-quarters of people living with these devices haven’t had conversations about what happens at end of life.
This communication gap creates problems. Nearly 40% of patients in one study thought withdrawing defibrillation therapy was equivalent to active euthanasia. This fundamental misunderstanding can prevent people from making informed decisions aligned with their values.
Many patients also don’t understand that the device will continue shocking indefinitely unless someone turns it off. Some assume it has a built-in feature to recognize when someone is dying. It doesn’t.
Practical Aspects of Device Management
If someone decides they want their ICD deactivated, the process is straightforward. A healthcare provider uses a programmer—a specialized computer—to wirelessly communicate with the device and turn off the shock function.
This takes minutes. It’s painless and completely reversible if circumstances change.
The pacing function can remain active if needed to maintain adequate heart rate. This provides continued benefit without the risk of painful shocks.
Timing matters, though. Having this conversation when you’re hospitalized with end-stage illness is harder than discussing it proactively. Many experts recommend addressing device management preferences during routine follow-up visits, especially if health status changes.
What Happens to the Device After Death
Once death occurs, the ICD typically needs removal before cremation. The lithium battery can explode when exposed to crematorium temperatures, creating safety hazards.
Funeral homes and medical examiners handle this routinely. The device is either deactivated and removed before cremation, or it remains in place if burial is chosen.
Some families choose to donate the removed device. Organizations exist that refurbish ICDs for use in countries where access to these life-saving technologies is limited, though this practice involves complex ethical and regulatory considerations.
Device Recalls and Safety Concerns
The FDA has issued recalls for certain ICD models due to potential malfunctions. According to FDA communications, one recall affected 348,616 devices with distribution dates from October 13, 2017 to June 9, 2023 due to risk of low or no energy output.
The FDA identified this as a Class I recall—the most serious type. Use of affected devices may cause serious injuries or death.
These recalls highlight an important reality: ICDs are complex medical devices that can fail. While extremely reliable overall, they’re not perfect. This underscores why advance planning matters—including understanding what happens if the device malfunctions during end-of-life care.
| Consideration | Keep ICD Active | Deactivate Shock Function |
|---|---|---|
| Primary benefit | Prevents sudden cardiac death from arrhythmia | Avoids painful shocks during natural dying |
| Best for patients with | Stable condition, reasonable life expectancy | Terminal illness, end-stage heart failure, hospice care |
| Risk of shocks | May fire during end-of-life process | No shock risk |
| Pacing function | Remains active | Can remain active if needed |
| Reversibility | Can be deactivated anytime | Can be reactivated if circumstances change |
Starting the Conversation
So how do you bring this up with your healthcare team?
Start simple: “I’d like to understand what happens with my ICD as I get older or if I develop other serious health problems.”
Most cardiologists and electrophysiologists welcome these discussions. They recognize the importance of aligning device management with patient values and goals.
Questions to ask include:
- What would happen with my ICD if I developed a terminal illness?
- Can the shock function be turned off while keeping pacing active?
- Who makes the decision about deactivation?
- How quickly can the device be deactivated if needed?
- What should my family know about device management?
Document your preferences in advance directives. Many standard forms don’t specifically address ICDs, so adding a separate statement clarifies your wishes.
Include information about your device in your medical records and share it with family members who might need to advocate for you.
What Healthcare Providers Recommend
Medical organizations increasingly recognize the importance of advance care planning for ICD patients. Research in palliative care emphasizes that active management of ICDs, including timely discussions about deactivation, reduces the risk of distressing shocks at end of life.
Guidelines suggest these conversations should happen at several points: at the time of implantation, during routine follow-ups, when health status changes significantly, and when entering palliative or hospice care.
The goal isn’t to discourage ICD therapy. These devices provide tremendous benefit for appropriate patients. Rather, the goal is ensuring people understand the full picture—including what happens at the end of life—so they can make informed decisions.
Frequently Asked Questions
No. ICDs specifically prevent sudden cardiac death from ventricular arrhythmias. They don’t prevent death from heart failure progression, non-cardiac illnesses, or other causes. Research shows most ICD patients die from heart failure or non-cardiac causes rather than the arrhythmias the device treats.
Yes, unless it’s deactivated. The device can’t distinguish between a potentially reversible arrhythmia and one occurring during the natural dying process. Nearly 30% of ICD patients receive shocks at end of life, which don’t extend survival but can cause distress.
No. ICD deactivation is a medical decision to allow natural processes without technological interference. It’s comparable to choosing not to start dialysis or declining ventilator support. Major medical and ethics organizations recognize this distinction.
Yes. Healthcare providers can selectively turn off the defibrillation capability while maintaining pacing support for slow heart rhythms. This allows continued benefit without risk of painful shocks.
Ideally during routine follow-up visits, especially if your health status changes. Key times include diagnosis of terminal illness, entering hospice care, or development of advanced heart failure. Don’t wait until a crisis—planning ahead reduces stress.
The device typically needs removal before cremation because the lithium battery can explode at high temperatures. Funeral homes handle this routinely. If burial is chosen, the device can remain in place.
Yes, if you’ve documented this preference in advance directives or if you’re unable to make decisions and family members serve as healthcare proxies. This is why discussing and documenting preferences ahead of time matters.
Moving Forward
Living with an implantable cardioverter defibrillator means accepting that technology plays a role in your cardiac care. But it doesn’t mean surrendering control over end-of-life decisions.
Understanding what happens if you die with a defibrillator empowers better planning. These conversations aren’t morbid or pessimistic—they’re practical and compassionate.
Talk with your cardiologist or electrophysiologist about device management preferences. Document your wishes in advance directives. Share this information with family members.
The device that protects your life today doesn’t have to interfere with a peaceful death tomorrow. But that outcome requires proactive communication and planning.
Don’t be part of the 76% who never have this conversation. Start today.