Quick Summary: Stopping duloxetine suddenly can trigger antidepressant discontinuation syndrome, causing symptoms like dizziness, nausea, brain zaps, headaches, and mood changes. Research from the NIH documents cases of seizures and severe withdrawal when duloxetine is abruptly discontinued. Gradual tapering under medical supervision is essential to minimize withdrawal effects, which can last from days to several weeks depending on treatment duration.
Duloxetine, commonly known by its brand name Cymbalta, is a serotonin-noradrenaline reuptake inhibitor (SNRI) prescribed for depression, anxiety, nerve pain, and fibromyalgia. While it’s effective for many conditions, discontinuing this medication isn’t as simple as just stopping the pills.
When someone stops taking duloxetine abruptly—what medical professionals call “going cold turkey”—the body and brain can react strongly. The sudden absence of this medication disrupts the chemical balance that’s been maintained, sometimes for months or years.
Here’s what actually happens when duloxetine is discontinued without proper tapering.
Understanding Antidepressant Discontinuation Syndrome
Antidepressants can cause tolerance, dependence, and withdrawal syndromes. The medical term is antidepressant discontinuation syndrome, though this phrasing sometimes understates the severity of what patients experience.
SNRIs work by increasing serotonin and noradrenaline levels in the brain. These neurotransmitters regulate mood, pain perception, and numerous bodily functions. When duloxetine is taken regularly, the brain adapts to these elevated chemical levels.
Stop the medication suddenly? The brain doesn’t have time to readjust. This creates a chemical imbalance that manifests as withdrawal symptoms.
According to research published by the NIH, about 20% of patients develop antidepressant discontinuation syndrome following an abrupt stoppage of or marked reduction in the dose of an antidepressant taken continuously for one month. But that number varies significantly based on the specific medication, dosage, and duration of use.
Documented Cases of Severe Duloxetine Withdrawal
The NIH has documented serious cases of duloxetine withdrawal that go beyond typical discomfort. One case report describes a patient who experienced two generalized tonic-clonic seizures just two days after stopping duloxetine abruptly.
Another documented case involved status cataplecticus—recurrent episodes of sudden whole-body paralysis with preserved consciousness—induced by abrupt duloxetine withdrawal in a patient with narcolepsy type 1.
These aren’t common outcomes, but they demonstrate the potential severity of stopping this medication without medical guidance. The brain’s adaptation to SNRIs runs deep, affecting multiple neurotransmitter systems.
Common Duloxetine Withdrawal Symptoms
Most people won’t experience seizures or extreme reactions, but withdrawal symptoms are still distressing and can significantly impact daily functioning.
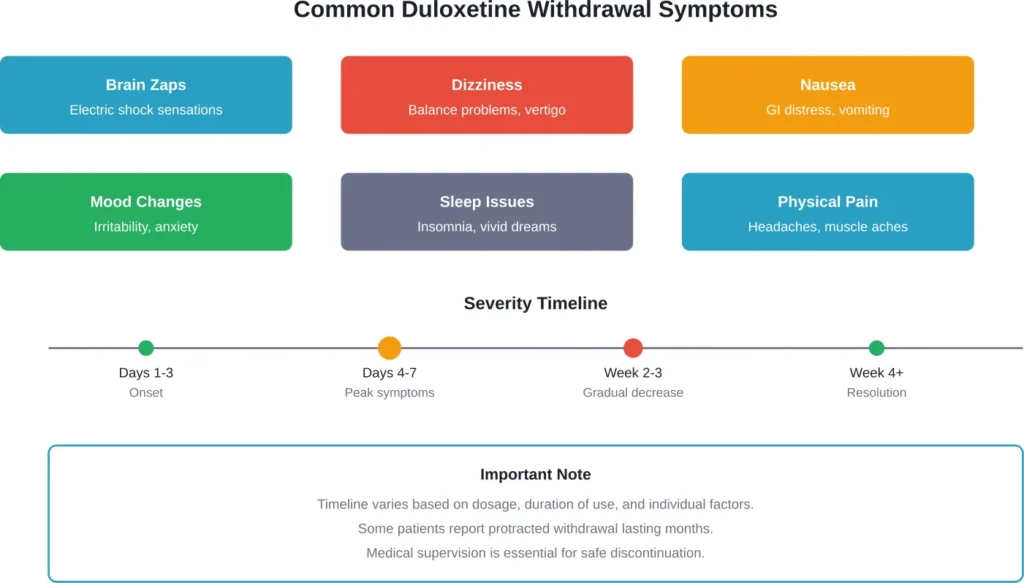
The most frequently reported duloxetine withdrawal symptoms include:
Brain Zaps and Neurological Symptoms
“Brain zaps” are one of the most distinctive and unsettling withdrawal effects. Patients describe them as electric shock sensations in the head, buzzing, or a feeling like the brain is “rebooting.”
Some patients describe brain zaps as a “noise in my head that never stops—buzz or electric,” according to community discussions.
These sensations aren’t dangerous, but they’re uncomfortable and can be alarming for people experiencing them for the first time.
Dizziness and Balance Issues
Dizziness ranks among the most common withdrawal symptoms. Some people report feeling unsteady, experiencing vertigo, or having difficulty with coordination.
One patient on Mayo Clinic Connect reported not trusting themselves to drive during withdrawal due to dizziness. The dizziness can be severe enough to impact work and daily activities.
Gastrointestinal Distress
Nausea is frequently reported during duloxetine withdrawal. Some people also experience vomiting, diarrhea, or general stomach upset.
The gut has a significant number of serotonin receptors, so changes in serotonin levels directly affect digestive function.
Mood and Emotional Changes
Irritability, anxiety, mood swings, and depression can intensify during withdrawal. For people who were taking duloxetine for depression or anxiety, these symptoms can be particularly concerning.
It’s sometimes difficult to distinguish between withdrawal symptoms and the return of the underlying condition being treated.
Sleep Disturbances
Insomnia, vivid dreams, and nightmares are commonly reported. Some people experience the opposite—excessive sleepiness and fatigue.
Some patients report experiencing multiple intense dreams during the withdrawal period, according to community discussions.
Physical Symptoms
Headaches, muscle aches, fatigue, sweating, and flu-like symptoms frequently accompany duloxetine withdrawal. Some people describe feeling like they have a severe cold or flu.
How Long Does Duloxetine Withdrawal Last?
The duration of withdrawal symptoms varies considerably. Symptoms typically begin within one to three days after the last dose.
Symptoms typically peak around day four to seven, then gradually diminish over the following weeks. The NHS notes that improvements may take longer for nerve pain patients.
But here’s where it gets complicated. Some patients report protracted withdrawal symptoms that persist for months. Community discussions on Mayo Clinic Connect include accounts of withdrawal effects lasting eight weeks or longer.
Several factors influence withdrawal duration:
- Dosage: Higher doses generally lead to more intense and prolonged withdrawal
- Duration of treatment: Longer treatment periods mean more significant brain adaptation
- Individual biochemistry: Genetic factors affect how quickly the body metabolizes medications
- Method of discontinuation: Abrupt cessation typically causes worse symptoms than gradual tapering
The Science Behind Why Withdrawal Happens
SNRIs like duloxetine work by blocking the reuptake of serotonin and noradrenaline. This means more of these neurotransmitters remain active in the brain’s synapses.
Over time, the brain adapts to this artificially elevated state. Receptor sensitivity changes, neurotransmitter production adjusts, and entire signaling pathways recalibrate.
When the medication is suddenly removed, those adaptations don’t instantly reverse. The brain is left in a state calibrated for high neurotransmitter levels but receiving much lower amounts.
This mismatch creates the constellation of symptoms known as withdrawal or discontinuation syndrome. The brain essentially needs time to readjust to functioning without the medication.
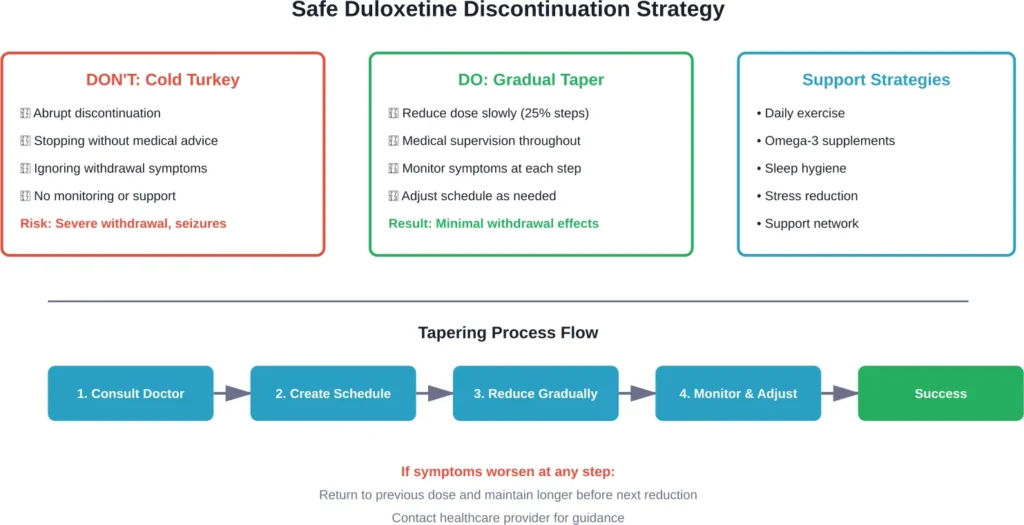
Safe Tapering: The Recommended Approach
Medical professionals universally recommend gradual tapering rather than abrupt discontinuation. Research has found that the rate of antidepressant tapering affects the incidence of discontinuation symptoms.
A typical tapering schedule might look like this:
| Week | Dosage Adjustment | Notes |
|---|---|---|
| 1-2 | Reduce by 25% | Monitor for symptoms |
| 3-4 | Reduce by another 25% | Stabilize at this level |
| 5-6 | Reduce by another 25% | Symptoms may emerge |
| 7-8 | Final reduction to zero | Close monitoring essential |
This is just one example. Some patients require slower tapers, especially those who’ve been on duloxetine for years or at higher doses. One patient described weaning from 120mg to zero over an 8 week period.
The key principle? Go slow enough that the brain can adapt gradually. If symptoms emerge during tapering, the current dose should be maintained longer before the next reduction.
Managing Withdrawal Symptoms When They Occur
Even with proper tapering, some withdrawal symptoms may still occur. Several strategies can help manage them:
Medical Interventions
Healthcare professionals might recommend:
- Slowing the taper schedule if symptoms are severe
- Temporarily increasing the dose then tapering more gradually
- Switching to a longer-acting antidepressant before tapering
- Prescribing medications to manage specific symptoms
Lifestyle Support Strategies
Non-pharmaceutical approaches can provide significant relief. Community discussions highlight several effective strategies:
Regular physical activity, even just daily walking, helps regulate mood and neurotransmitter function. Exercise promotes natural endorphin production, which can partially compensate for the chemical changes during withdrawal.
Omega-3 fatty acids may support brain function during the transition. Some patients report benefits from high-quality fish oil supplements.
Sleep hygiene becomes especially important. Maintaining consistent sleep and wake times, even when experiencing insomnia, helps the brain establish new rhythms.
Stress reduction techniques—meditation, deep breathing, progressive muscle relaxation—can help manage anxiety and irritability.
Symptom-Specific Relief
For brain zaps: These typically can’t be eliminated but often decrease with time. Staying hydrated and avoiding sudden head movements may reduce frequency.
For nausea: Small, frequent meals and ginger tea can help. Anti-nausea medications may be prescribed if symptoms are severe.
For dizziness: Moving slowly when changing positions, staying hydrated, and avoiding driving during peak symptoms are important safety measures.
When to Seek Immediate Medical Attention
Most withdrawal symptoms, while uncomfortable, aren’t medically dangerous. But certain symptoms require immediate medical evaluation:
- Seizures or convulsions
- Suicidal thoughts or behaviors
- Severe confusion or disorientation
- Chest pain or rapid heartbeat
- Extreme agitation or panic attacks
- Hallucinations or delusions
Research from the NIH documents that while rare, seizures can occur with abrupt duloxetine discontinuation. Any neurological symptoms warrant immediate evaluation.
Akathisia—a severe form of restlessness and agitation—can also emerge during withdrawal and may increase suicide risk. This requires prompt medical intervention.
Special Considerations for Long-Term Users
People who’ve taken duloxetine for years face unique challenges when discontinuing. The brain’s adaptations are more entrenched, and the withdrawal process often needs to be more gradual.
For someone who’s been on duloxetine for five or ten years, an eight-week taper might not be sufficient. Some long-term users require tapers lasting six months or longer.
The phenomenon of protracted withdrawal is more common in long-term users. Some patients report lingering symptoms—typically mood changes, sleep disturbances, or cognitive issues—that persist for months after the medication is completely discontinued.
Why People Stop Taking Duloxetine
Understanding why someone wants to discontinue duloxetine can inform the approach. Common reasons include:
- Side effects that outweigh benefits
- Feeling better and wanting to try managing without medication
- Sexual dysfunction caused by the medication
- Weight gain or metabolic concerns
- Pregnancy planning
- Switching to a different medication
- Financial considerations
Each situation requires a tailored discontinuation plan. Someone switching to another antidepressant might cross-taper, gradually decreasing duloxetine while increasing the new medication. Someone who’s in remission might taper more conservatively to minimize relapse risk.
The Role of Healthcare Providers
Medical supervision isn’t optional when discontinuing duloxetine—it’s essential. Healthcare providers can:
- Assess overall health status and medication history
- Create an individualized tapering schedule
- Monitor for withdrawal symptoms and underlying condition relapse
- Adjust the plan if symptoms become problematic
- Prescribe supportive medications if needed
- Provide referrals to mental health professionals for additional support
The withdrawal process should be collaborative. Patients should report all symptoms, even minor ones, so providers can gauge how the taper is progressing.
Distinguishing Withdrawal from Relapse
One of the trickiest aspects of duloxetine discontinuation is distinguishing withdrawal symptoms from relapse of the original condition.
Depression and anxiety symptoms can emerge during withdrawal that mimic the conditions duloxetine was treating. How can someone tell the difference?
Timing provides clues. Withdrawal symptoms typically begin within days of dose reduction and improve over weeks. Relapse symptoms tend to develop more gradually and worsen over time rather than improving.
The specific symptom profile also differs. Brain zaps, dizziness, and flu-like symptoms point toward withdrawal. A gradual return of persistent sadness, loss of interest, or chronic pain suggests potential relapse.
Healthcare providers can help make this distinction and determine whether the taper should continue or if treatment needs to be reconsidered.
Frequently Asked Questions
Duloxetine withdrawal itself is rarely life-threatening, but severe complications can occur. The NIH has documented cases of seizures from abrupt duloxetine discontinuation. Extreme cases of akathisia may increase suicide risk. Medical supervision significantly reduces these risks.
Tapering duration varies based on dosage, treatment length, and individual response. Typical tapers range from 4-8 weeks, but long-term users may require several months. Research suggests slower tapers reduce discontinuation symptoms. Work with a healthcare provider to determine the appropriate timeline.
Even short-term use can require tapering. Brain chemistry changes begin quickly after starting SNRIs. Consult the prescribing physician before stopping, even after brief treatment. They may recommend a shorter taper or determine that abrupt discontinuation is safe in specific cases.
Brain zaps are uncomfortable but not dangerous and don’t cause permanent neurological damage. They’re a temporary symptom of neurotransmitter readjustment. Most people find they completely resolve within weeks of completing the taper, though they can persist longer in some cases.
Protracted withdrawal can occur, with symptoms persisting for months. If symptoms remain severe or interfere with daily functioning beyond the expected timeframe, consult a healthcare provider. They may recommend reinstating a low dose and tapering more gradually, or investigate whether symptoms represent a relapse of the underlying condition.
Alternating-day dosing isn’t recommended for duloxetine. This approach creates fluctuating blood levels that can worsen withdrawal symptoms. Instead, reduce the daily dose gradually. Some physicians prescribe lower-dose capsules or use compounding pharmacies to create custom doses for smoother tapering.
Alcohol should be avoided or minimized during withdrawal. It affects the same neurotransmitter systems already disrupted by duloxetine discontinuation, potentially worsening mood symptoms and intensifying withdrawal effects. Alcohol can also interfere with sleep quality, which is often already compromised during withdrawal.
Moving Forward After Duloxetine
Successfully discontinuing duloxetine is achievable with proper planning and support. The key is patience—rushing the process increases suffering and failure risk.
Most people who taper gradually under medical supervision navigate withdrawal successfully, though not always comfortably. The temporary discomfort of a well-managed taper beats the potential severity of abrupt discontinuation.
For those discontinuing because they feel better, remember that symptom management doesn’t end when the medication does. Continuing therapy, maintaining healthy lifestyle habits, and staying connected to support systems remain important.
For those switching medications, the transition period requires close monitoring. The new medication may take weeks to reach full effectiveness while duloxetine is being reduced.
And for those who discover during tapering that they’re not ready to stop, that’s okay too. There’s no shame in recognizing that continued treatment is the right choice. The attempt provides valuable information about medication needs.
The decision to stop duloxetine should always be made collaboratively with healthcare providers. They can assess individual circumstances, create appropriate discontinuation plans, and provide support throughout the process.
Abruptly stopping this medication carries real risks documented by medical research. But with proper tapering, medical supervision, and patience, most people can successfully discontinue duloxetine and move forward with their treatment journey.