
Quick Summary: Taking melatonin every night is generally safe for short-term use, but long-term nightly use may reduce effectiveness and could impact natural melatonin production. Recent studies suggest potential concerns with extended use, including possible links to heart health issues. For chronic sleep problems, cognitive behavioral therapy and sleep hygiene improvements offer safer, more sustainable alternatives.
Melatonin has become the fourth most popular natural supplement taken by adults in the United States. If you’ve reached for that little bottle on your nightstand more times than you can count, you’re part of a growing trend. Between 1999 and 2018, usage jumped from 0.4% to 2.1% of American adults.
But here’s the thing—just because something is natural doesn’t mean it’s harmless to use indefinitely. The question isn’t whether melatonin works. It’s whether your nightly habit is doing more harm than good.
Understanding Melatonin: The Sleep Hormone
According to the National Center for Complementary and Integrative Health (NCCIH), melatonin is a hormone that your brain produces in response to darkness. It helps regulate your circadian rhythms—that 24-hour internal clock that tells your body when to sleep and wake.
Light exposure at night blocks melatonin production. That’s why scrolling through your phone at midnight isn’t doing you any favors.
Research suggests melatonin plays other important roles beyond sleep regulation, though these effects aren’t fully understood. What we do know is that supplemental melatonin can help with specific sleep disorders, particularly delayed sleep-wake phase disorder (DSWPD).
A 2016 review that looked at a small number of people (52) from two studies showed that melatonin supplements reduced the time it took for people with DSWPD to fall asleep by about 22 minutes on average compared to placebo. Not bad for people with DSWPD—but that doesn’t mean everyone should pop it nightly.
Short-Term vs. Long-Term Melatonin Use
Melatonin is safe for short-term use. Most studies focus on periods ranging from a few days to several months. For jet lag, occasional shift work, or temporary sleep disruptions, melatonin can be remarkably effective.
A 2002 Cochrane review found melatonin particularly effective for alleviating jet lag after traveling across multiple time zones. Occasional short-term use appears to carry minimal risk.
Long-term nightly use? That’s where things get complicated.
What Happens to Your Natural Production
One major concern with chronic melatonin use is whether it suppresses your body’s natural production. The research here is somewhat reassuring—a study published in PubMed found that a physiological dose of 0.5 mg given to night shift workers for seven days didn’t affect the amplitude of endogenous melatonin secretion.
That said, most people take far more than 0.5 mg. Many supplements contain 3-10 mg, well above physiological levels.
Real talk: the long-term impact of supraphysiological doses on natural melatonin production is not well established. Some research suggests effectiveness diminishes after chronic use in certain populations, including hemodialysis patients.
The Tolerance Question
Does your body build tolerance to melatonin? Evidence suggests it might.
Studies on hemodialysis patients found that the sleep-promoting effects of exogenous melatonin diminished after long-term use. After a “melatonin holiday,” circadian melatonin rhythms recovered, suggesting the body may adapt to chronic supplementation.
This means if you’ve been taking melatonin every night for months and wondering why it doesn’t work like it used to, tolerance could be the culprit.
Recent Research: Heart Health Concerns
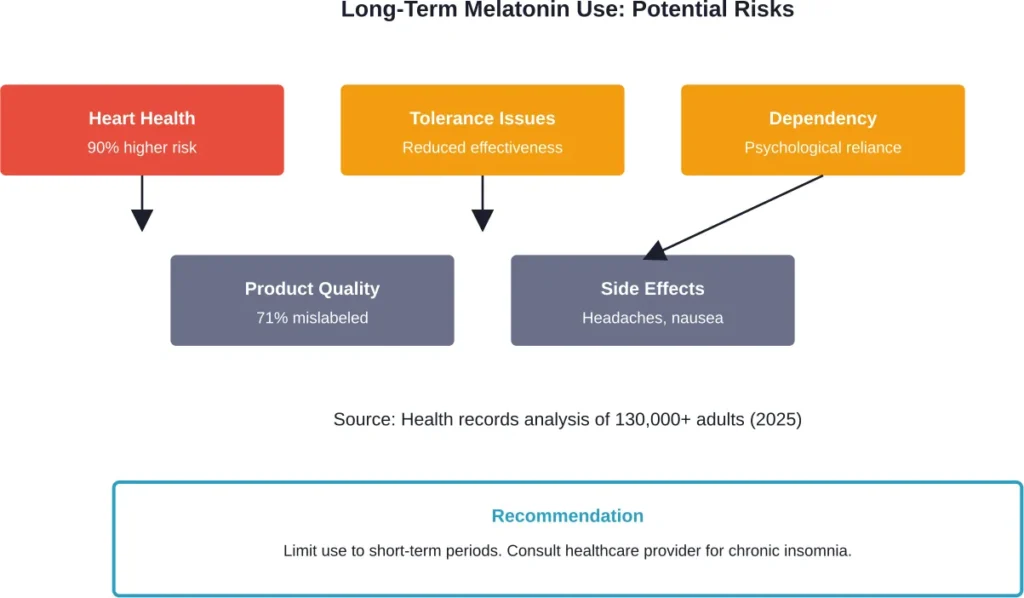
A 2025 review presented at the American Heart Association Scientific Sessions analyzed five years of health records for more than 130,000 adults with insomnia who used melatonin for at least one year. The findings raised concerns.
Among adults with insomnia, those whose electronic health records indicated long-term melatonin use (12 months or more) had about a 90% higher chance of incident heart failure over five years compared to those without such indication. They also faced increased risks for hospitalization related to the condition.
Now, this doesn’t prove melatonin causes heart failure. People taking melatonin long-term likely have underlying health issues contributing to both insomnia and cardiovascular risk. But it’s a red flag worth discussing with your doctor.
Common Side Effects of Regular Melatonin Use
Even short-term melatonin use can produce side effects. The most common include:
- Headaches
- Dizziness
- Nausea
- Drowsiness during the day
Less common but documented side effects include anxiety, irritability, and vivid dreams or nightmares. Some people experience stomach cramps or temporary feelings of depression.
These effects tend to be mild and resolve when you stop taking the supplement. But when you’re using it every single night, those “mild” annoyances can add up.
The Supplement Quality Problem
Here’s something most people don’t know: melatonin supplements are wildly inconsistent.
A 2017 study published in the Journal of Clinical Sleep Medicine examined melatonin supplement content and found that melatonin content did not meet within a 10-percent margin of the label claim in more than 71 percent of supplements, with the actual content ranging from 83 percent less to 478 percent more than the concentration declared on the label.
A 2023 study on over-the-counter melatonin gummies found accuracy issues. In these products, the actual quantity of melatonin ranged from 74-347% of the labeled quantity, with researchers finding that 22 of the 25 products (88%) were inaccurately labeled.
So when you think you’re taking 3 mg, you might actually be getting 0.5 mg—or 14 mg. That’s not exactly reassuring for a nightly habit.
| Study | Products Tested | Inaccurately Labeled | Content Range |
|---|---|---|---|
| 2017 JCSM Study | 31 supplements | 71% | -83% to +478% |
| 2023 Gummy Study | 25 gummies | 88% | 74% to 347% |
Melatonin Dosage: How Much Is Too Much?
Most people take way more melatonin than necessary. Physiological doses range from 0.3 mg to 1 mg. Many over-the-counter supplements contain 3 mg, 5 mg, or even 10 mg.
Higher doses don’t necessarily work better. In fact, they may increase side effects without improving sleep quality.
Studies showing effectiveness typically used doses between 0.5 mg and 3 mg, taken 30 minutes to an hour before bedtime. Starting with the lowest effective dose makes sense, especially for nightly use.
Special Considerations: Children and Melatonin
Melatonin use in children has skyrocketed. Research suggests that as many as 6% of children, i.e., over 4 million children, take melatonin at least monthly.
According to Harvard Health and the American Academy of Sleep Medicine (AASM), melatonin isn’t regulated by the FDA as a medication. This raises concerns about quality control and appropriate dosing in developing children.
For kids struggling with sleep, behavioral interventions should come first. These include:
- Consistent bedtime routines
- Limiting screen time 30-60 minutes before bed
- Maintaining regular sleep schedules
- Creating a dark, cool sleep environment
If melatonin is necessary, it should be used under medical supervision and not as a nightly, indefinite solution.
Safer Alternatives for Chronic Sleep Problems
Look, melatonin has its place. But if you’ve been relying on it every night for months, it’s time to explore better options.
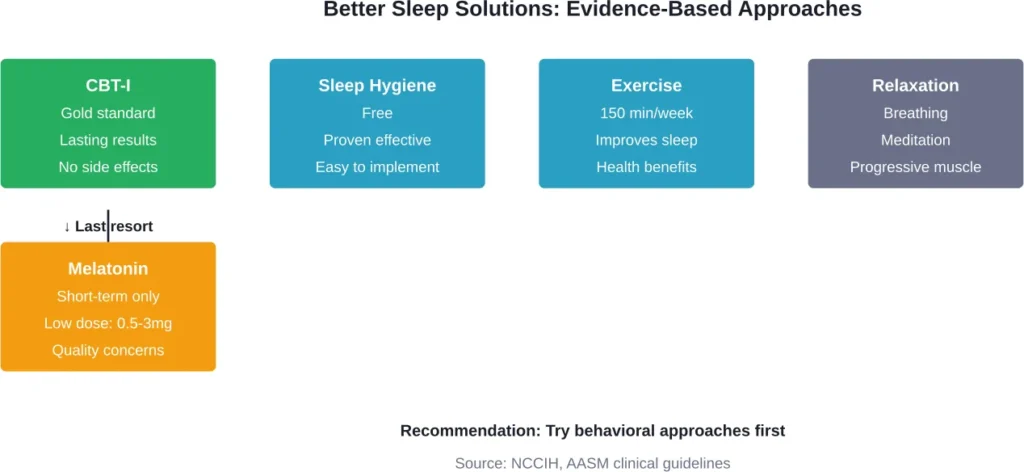
Cognitive Behavioral Therapy for Insomnia (CBT-I)
CBT-I is the undisputed first-line therapy for insomnia with lasting results. Traditionally 4-8 in person sessions with therapist, it’s now available via phone, internet platforms, and self-help books.
Research shows these alternative delivery methods produce similar results to traditional therapy. Options like SHUTi, Sleepio, and Sleepstation offer evidence-based treatment without the need for medication.
Sleep Hygiene Improvements
Sleep hygiene sounds boring, but it works. Key practices include:
- Maintaining consistent sleep and wake times, even on weekends
- Keeping your bedroom dark, quiet, and cool (around 65-68°F)
- Avoiding caffeine after 2 PM
- Limiting alcohol, which disrupts sleep architecture
- Getting regular exercise—experts recommend adults exercise about 150 minutes per week
Listening to music may promote relaxation before bed. So can reading (actual books, not screens).
Relaxation Techniques
The NCCIH notes that relaxation techniques are sometimes included in CBT-I protocols. While evidence quality is lower than for full CBT-I, techniques like progressive muscle relaxation, deep breathing exercises, and meditation may help certain people with insomnia.
These approaches don’t carry the risks or quality control issues of supplements.
When to Talk to Your Doctor
If sleep problems persist for more than a few weeks, see a healthcare provider. Chronic insomnia often has underlying causes that melatonin won’t fix.
Conditions that can disrupt sleep include:
- Obstructive sleep apnea
- Restless leg syndrome
- Chronic pain
- Anxiety and depression
- Certain medications
Treating the root cause beats masking symptoms with supplements.
Additionally, if you’ve been taking melatonin nightly for months and want to stop, talk to your doctor about the best approach. Some people experience rebound insomnia when discontinuing after long-term use.
The Bottom Line on Nightly Melatonin Use
Taking melatonin every night isn’t inherently dangerous for most adults in the short term. But the evidence doesn’t support it as a safe, effective long-term solution for chronic insomnia.
Tolerance can develop. Natural production may be affected. Quality control is inconsistent at best. And recent research raises questions about cardiovascular risks with extended use.
For occasional jet lag, shift work adjustments, or temporary sleep disruptions, melatonin works well. For chronic sleep problems, behavioral interventions like CBT-I and sleep hygiene improvements offer better, safer, more sustainable results.
The supplement aisle offers quick fixes. Real sleep health requires a different approach.
Frequently Asked Questions
Melatonin doesn’t cause physical addiction like some sleep medications. However, psychological dependence can develop where someone feels unable to sleep without it. The body may also build tolerance over time, requiring higher doses for the same effect.
Melatonin has a relatively short half-life of about 40-60 minutes in most people. It’s typically cleared from the body within 4-5 hours. However, timing matters—taking it too early or too late can disrupt your natural circadian rhythm.
Taking melatonin only when needed for specific situations—like jet lag, occasional insomnia, or shift work—is safer than nightly use. This approach reduces the risk of tolerance, maintains effectiveness, and avoids potential long-term health concerns.
Studies show effective doses typically range from 0.5 mg to 3 mg taken 30-60 minutes before bedtime. Starting with the lowest dose (0.5-1 mg) is recommended. Higher doses don’t necessarily improve sleep quality and may increase side effects.
Yes. Melatonin can interact with blood thinners, immunosuppressants, diabetes medications, and birth control pills. It may also enhance the effects of sedatives and anticonvulsants. Always consult a healthcare provider before combining melatonin with prescription medications.
Melatonin doesn’t cause physical withdrawal symptoms like some sleep medications. However, some people experience temporary rebound insomnia when stopping after months of nightly use. Gradually reducing the dose rather than stopping abruptly may help.
Research suggests the body can develop tolerance to melatonin after chronic use, particularly at higher doses. Studies on hemodialysis patients showed diminished sleep-promoting effects after long-term use, which improved after a break from supplementation.