
Quick Summary: Natural pregnancy after menopause is virtually impossible because ovulation has permanently ceased. However, postmenopausal women can achieve pregnancy through assisted reproductive technologies like IVF with donor eggs, though this carries significantly elevated health risks.
The question of pregnancy after menopause confuses many women. Hot flashes, irregular periods, mood changes—these symptoms blur the line between perimenopause and actual menopause. And that confusion creates real uncertainty about fertility.
Here’s the thing though: understanding where you are in the menopausal transition dramatically affects family planning decisions. The answer isn’t simply yes or no. It depends on which stage you’re in and what type of pregnancy we’re discussing.
According to the World Health Organization, after menopause, a woman cannot become pregnant naturally, except in rare cases when specialized fertility treatments are used. But what counts as “after menopause”? And what do those specialized treatments actually involve?
Understanding Menopause vs. Perimenopause
Most women experience menopause between ages 45 and 55 as a natural biological process. But menopause isn’t a sudden switch. It’s one specific point in a continuum.
Menopause is officially confirmed after 12 consecutive months without a menstrual period. That’s the clinical definition. Until you’ve hit that 12-month mark, you’re technically still in perimenopause—the transitional phase leading up to menopause.
Perimenopause can last anywhere from a few months to several years. During this time, hormonal changes cause irregular periods, but ovulation still happens occasionally. And that’s where pregnancy remains possible.
The Three Distinct Stages
The menopausal transition breaks down into three phases:
- Perimenopause: Irregular periods, fluctuating hormones, intermittent ovulation
- Menopause: The specific day marking 12 months since your last period
- Postmenopause: Everything after that 12-month mark
Pregnancy risk exists during perimenopause but essentially disappears in postmenopause. That distinction matters enormously.
Fertility Decline With Age: What the Numbers Show
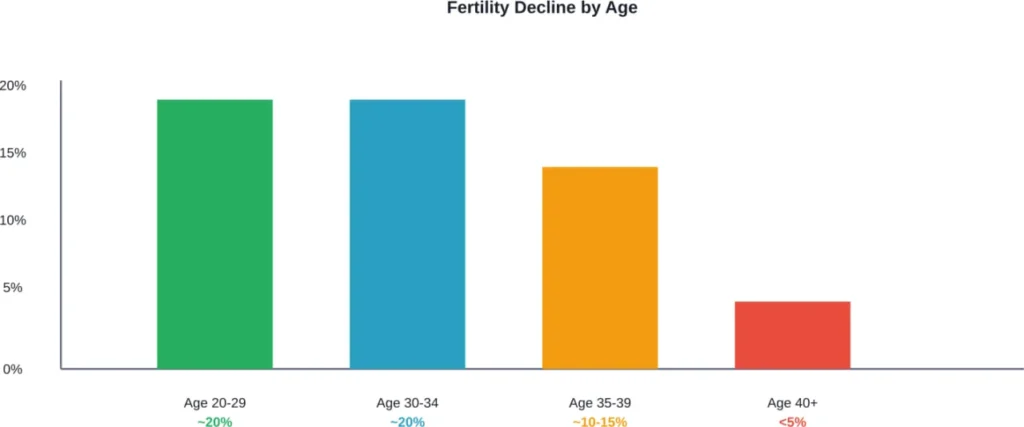
Female fertility doesn’t crash overnight. It’s a gradual decline that accelerates after age 35.
For healthy couples in their 20s or early 30s, the chance that a woman will get pregnant is about 25 to 30 percent in any single menstrual cycle. By age 30, fertility begins to decline. By age 40, that drops below 5% per month. The aging ovaries produce fewer eggs, and the quality of those eggs deteriorates.
According to ACOG data from a 1982 study evaluating success with donor sperm insemination, the pregnancy rate with up to 12 months of insemination cycles decreased from 74% for individuals younger than age 31 years, to 62% for those aged 31–35 years, and 54% for those older than age 35 years.
This decline happens because women are born with a finite number of eggs. Unlike men who continually produce sperm, female egg count only decreases over time. By menopause, the ovarian reserve is functionally depleted.
Can You Get Pregnant Naturally After Menopause?
The short answer? No.
True menopause means ovulation has permanently stopped. Without ovulation, there’s no egg to fertilize. Natural conception requires a released egg, and postmenopausal ovaries don’t release eggs.
But here’s where confusion creeps in. During perimenopause—before that official 12-month mark—ovulation still occurs sporadically. Periods become irregular, sometimes absent for months, then suddenly return. That unpredictability means pregnancy remains possible.
Real talk: if you haven’t completed a full year without menstruation, you’re not postmenopausal yet. Birth control still matters if pregnancy isn’t desired.
The Perimenopause Window
Perimenopause is the wild card. Hormonal fluctuations during this phase cause:
- Irregular menstrual cycles
- Unpredictable ovulation
- Difficulty tracking fertile windows
- False assumptions about fertility loss
Some women assume missed periods mean pregnancy is impossible. Then ovulation happens unexpectedly, and conception occurs. These “surprise” pregnancies during perimenopause aren’t uncommon.
Medical professionals typically recommend continuing contraception until 12 months post-final-period if pregnancy prevention is the goal.
Assisted Reproductive Technology: IVF After Menopause
Now this is where it gets interesting. While natural pregnancy after menopause isn’t possible, assisted reproductive technologies have changed what’s medically feasible.
Research published in medical journals confirms that women over age 50 and up to 62 can become pregnant using donated oocytes (eggs). The aging uterus, when treated with hormone replacement therapy, allows embryo implantation comparably to younger women.
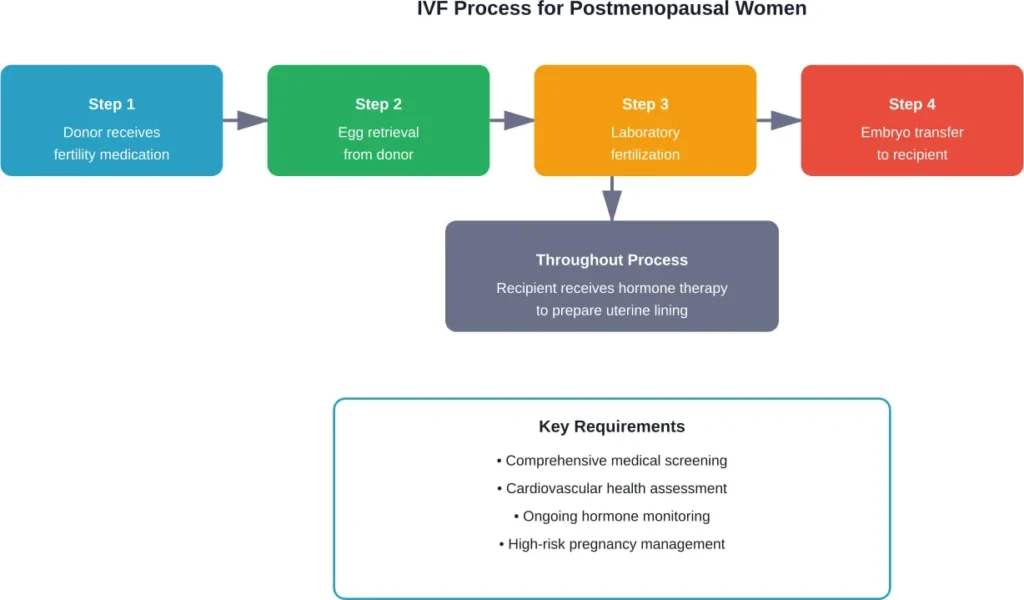
How IVF With Donor Eggs Works
The process involves several steps:
- A younger woman (the donor) takes fertility medications to stimulate egg production
- Eggs are retrieved during minor surgery
- The eggs are fertilized with sperm in a laboratory
- Resulting embryos are transferred to the recipient’s uterus
- Hormone therapy supports the uterine lining for implantation
The postmenopausal woman receives hormonal treatment to prepare her uterus for pregnancy. The embryo doesn’t contain her genetic material—it comes from the donor egg—but she carries and delivers the pregnancy.
Medical case reports document postmenopausal pregnancy via oocyte (egg) donation, with documented cases including women in advanced age. It’s physiologically possible, though increasingly controversial as maternal age climbs.
Health Risks of Postmenopausal Pregnancy
Look, just because something is medically possible doesn’t mean it’s medically advisable. Pregnancy after menopause—whether during late perimenopause or via IVF—carries substantially elevated risks.
According to ACOG data from 2020, nearly 19% of all pregnancies and 11% of all first pregnancies in the United States were in women aged 35 years and older. Advanced maternal age increases complications. And postmenopausal pregnancy pushes those risks even higher.
Maternal Health Complications
Medical case reports document serious complications in postmenopausal pregnancies:
- Chronic hypertension and preeclampsia: Blood pressure problems escalate dramatically
- Gestational diabetes: Glucose regulation becomes more difficult with age
- Cardiovascular strain: The heart works harder during pregnancy; aging hearts struggle more
- Placental complications: Placenta previa and placenta accreta occur more frequently
- Antepartum hemorrhage: Dangerous bleeding before delivery
A documented case of a 65-year-old postmenopausal woman presented with chronic hypertension, gestational diabetes, valvular heart disease, and placenta previa. These aren’t minor inconveniences—they’re life-threatening conditions.
Pregnancy Loss and Complications
Miscarriage risk increases with maternal age. The older the mother, the higher the likelihood of chromosomal abnormalities in embryos, even with donor eggs (though donor egg age matters more than recipient age for genetic issues).
Preterm birth rates climb. Cesarean delivery becomes more likely. Recovery takes longer. The physical demands of pregnancy strain an aging body in ways they wouldn’t affect a younger woman.
| Risk Factor | Young Mothers | Advanced Maternal Age | Postmenopausal |
|---|---|---|---|
| Gestational Diabetes | Lower risk | Moderate risk | Significantly elevated |
| Hypertensive Disorders | Lower risk | Increased risk | High risk |
| Cesarean Delivery | Lower rate | Higher rate | Very high rate |
| Placental Complications | Lower risk | Moderate risk | Elevated risk |
| Cardiovascular Strain | Well-tolerated | More challenging | Potentially dangerous |
Ethical Considerations and Medical Guidelines
The medical community remains divided on postmenopausal pregnancy. Physicians balance professional autonomy against patient autonomy—respecting a woman’s right to choose while acknowledging medical risks.
Many fertility clinics set age limits for assisted reproductive procedures. These limits vary, but commonly fall between 50-55 years. Some refuse treatment beyond certain ages based on safety concerns.
Research published in medical ethics journals explores these dilemmas. One paper asks directly: how old is too old for assisted reproductive technology? There’s no universal consensus.
Arguments supporting access emphasize reproductive freedom and women’s autonomy. Arguments against cite maternal health risks, the child’s welfare (considering parental age and longevity), and healthcare resource allocation.
Pregnancy During Perimenopause: A Different Scenario
Perimenopause deserves separate consideration. This isn’t postmenopausal pregnancy—it’s pregnancy during the transition to menopause.
Natural conception still occurs during perimenopause, though unpredictably. Women in their late 40s and early 50s sometimes assume they’re infertile when they’re not. Irregular cycles create false security.
Recognizing the Difference
How do you know if you’re perimenopausal versus postmenopausal? The 12-month rule applies. Until a full year passes without menstruation, perimenopause continues and pregnancy remains theoretically possible.
Symptoms overlap significantly:
- Hot flashes
- Night sweats
- Mood changes
- Irregular bleeding
- Sleep disturbances
But perimenopause includes occasional periods and sporadic ovulation. Postmenopause means permanent cessation.
Birth Control Considerations
If pregnancy isn’t desired, contraception remains necessary during perimenopause. Healthcare providers typically recommend continuing birth control for 12 months after the last period for women over 50, or 24 months for women under 50.
That said, perimenopause pregnancy carries its own elevated risks similar to advanced maternal age—just not as extreme as postmenopausal IVF pregnancy.
When to Consult a Healthcare Provider
Certain situations absolutely require professional medical guidance:
- Vaginal bleeding after confirmed menopause (12+ months without periods)
- Uncertainty about menopausal status and pregnancy possibility
- Interest in fertility preservation before menopause
- Considering assisted reproductive technology after menopause
- Unexplained symptoms during perimenopause
Postmenopausal bleeding can indicate serious conditions beyond pregnancy—including endometrial atrophy, polyps, or endometrial cancer. Medical evaluation is essential.
According to medical case reports, various diseases may lead to vaginal bleeding during menopause, which serves as an alarm for both patients and healthcare providers. Don’t assume bleeding means pregnancy; get it checked.
Fertility Preservation Options
Women approaching menopause who want future pregnancy options can consider fertility preservation. This involves freezing eggs or embryos before menopause depletes the ovarian reserve.
Egg freezing works best in younger women. By the time perimenopause begins, egg quality and quantity have already declined significantly. Still, it’s an option worth discussing with a fertility specialist if future pregnancy is desired.
The process mirrors IVF’s initial steps: hormone stimulation, egg retrieval, then freezing for later use. When pregnancy is desired, frozen eggs are thawed, fertilized, and transferred.
Alternative Paths to Motherhood
Postmenopausal women seeking to become mothers have options beyond pregnancy:
- Adoption: Building a family without pregnancy-related health risks
- Fostering: Providing care and stability for children in need
- Surrogacy: Using a gestational carrier with the intended mother’s frozen eggs (if preserved earlier) or donor eggs
These paths avoid the medical complications associated with postmenopausal pregnancy while still achieving motherhood.
Frequently Asked Questions
No. Menopause, by definition, means ovulation has permanently stopped. The ovaries have depleted their egg supply and no longer release eggs. If ovulation still occurs occasionally, you’re in perimenopause, not true menopause.
Bleeding after 12 months of no periods isn’t necessarily menstruation—it could indicate a medical problem. Postmenopausal bleeding requires immediate evaluation to rule out conditions like endometrial cancer, polyps, or atrophy. Schedule an appointment with a healthcare provider promptly.
Many fertility centers set age limits that may exclude postmenopausal women. Consultation with fertility clinics directly will provide information about availability and current policies, as these change frequently.
Pregnancy after 50 carries substantially elevated health risks, including hypertensive disorders, gestational diabetes, cardiovascular complications, and placental problems. While medically possible with assisted reproductive technology, it requires extensive screening, monitoring, and management by specialists experienced in high-risk pregnancies.
Hormone replacement therapy can cause withdrawal bleeding similar to periods, but it doesn’t restore fertility or restart ovulation in postmenopausal women. The ovarian egg supply has been depleted and cannot be replenished with hormones.
Medical guidelines typically recommend continuing contraception for 12 months after the last period for women over age 50, or 24 months for women under 50. This ensures you’ve truly reached menopause before discontinuing pregnancy prevention.
Documented cases of natural conception after confirmed menopause are extremely rare and often involve diagnostic errors—the woman was actually in late perimenopause, not true postmenopause. Once ovarian function has permanently ceased, natural conception is not possible.
Final Thoughts
The boundary between possible and advisable matters here. Postmenopausal pregnancy through assisted reproductive technology is technically feasible. Women in their 50s and 60s have successfully carried pregnancies using donor eggs.
But feasibility doesn’t equal safety. The medical risks escalate dramatically with maternal age. Cardiovascular complications, hypertensive disorders, gestational diabetes, and placental problems occur at much higher rates. These aren’t minor inconveniences—they’re serious, potentially life-threatening conditions.
Natural pregnancy after true menopause simply doesn’t happen. Ovulation has permanently stopped. The reproductive window has closed. During perimenopause, pregnancy remains possible but unpredictable.
If you’re navigating perimenopause, menopause, or considering postmenopausal pregnancy options, comprehensive medical guidance is essential. Every situation is unique. Age, overall health, medical history, and individual circumstances all factor into safe decision-making.
Don’t navigate this alone. Schedule a consultation with an obstetrician-gynecologist or reproductive endocrinologist. Discuss your specific situation, understand your risks, and explore all available options—including alternatives to pregnancy if health concerns make it inadvisable.
Your reproductive journey doesn’t have to end with menopause, but the path forward requires careful planning, honest medical assessment, and realistic expectations about both possibilities and limitations.