
Quick Summary: Walking with posterior tibial tendonitis is generally acceptable if pain levels remain manageable and proper precautions are taken. Rest is crucial during acute flare-ups, but complete immobilization isn’t typically necessary for most cases. A balanced approach combining controlled activity, supportive footwear, orthotic devices, and gradual rehabilitation exercises offers the best path to recovery.
The question of whether to walk with posterior tibial tendonitis sparks considerable debate—and for good reason. This condition, which affects the tendon supporting your foot’s medial arch, demands a nuanced approach to activity management.
Getting the balance wrong can prolong recovery. Push too hard, and pain escalates. Rest too much, and weakness develops.
The short answer? Walking isn’t automatically off-limits, but context matters enormously.
Understanding Posterior Tibial Tendonitis
Posterior tibial tendonitis involves inflammation and degeneration of the posterior tibial tendon, which runs along the inside of your ankle and connects to several bones in your foot’s arch. This tendon serves as the primary dynamic stabilizer of the medial longitudinal arch during gait.
The tibialis posterior muscle plays a critical role in supporting the arch during normal walking and gait.
The condition affects between 3.3%–10% of the population, with higher prevalence in specific demographics. Women in their 40s and 50s face elevated risk, and the classic patient profile includes females in their 6th decade of life who carry excess weight.
What Causes This Condition
Several factors contribute to posterior tibial tendon breakdown. Obesity plays a significant role—research shows that obesity represents a significant risk factor in progressive collapsing foot deformity, with the majority of patients carrying excess weight.
Other risk factors include hypertension, diabetes, previous trauma, and steroid exposure. The tendon can also contain a sesamoid bone or fibrocartilaginous structure at the navicular insertion point. The sesamoid functions as a pressure-absorbing or gliding mechanism and was found in approximately 23% of adult feet in anatomical studies.
Repetitive stress from activities that repeatedly load the arch—like running, hiking, or prolonged standing—gradually damages tendon fibers. The condition typically affects only one foot rather than both.
Recognizing the Symptoms
Pain along the inside of your ankle and arch represents the hallmark symptom. This discomfort typically worsens with activity and improves with rest.
Swelling frequently develops along the tendon’s path. Some patients notice a gradual flattening of the arch over time. Difficulty standing on tiptoe on the affected foot signals significant tendon weakness.
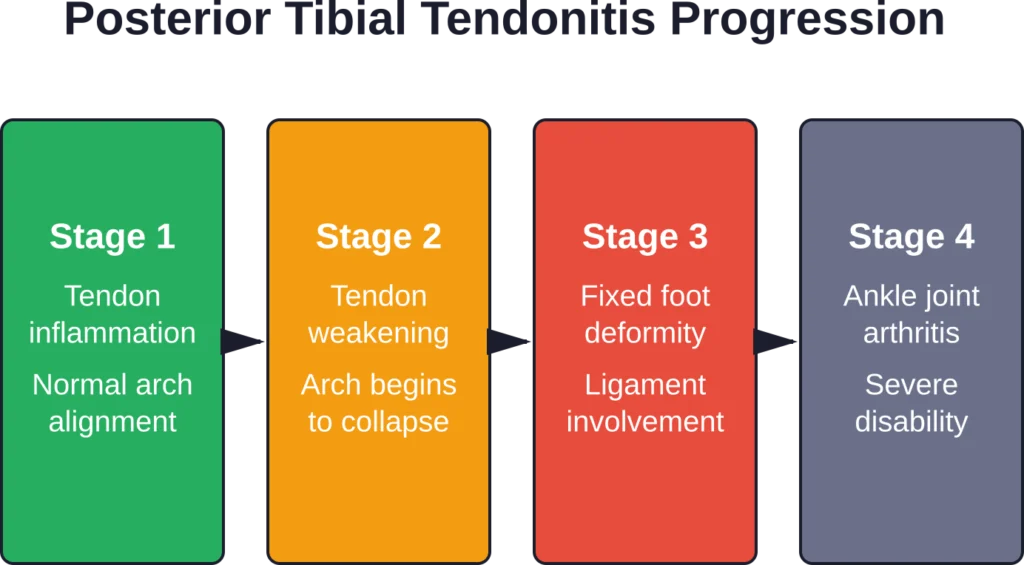
The condition progresses through distinct stages if left untreated, eventually leading to posterior tibial tendon dysfunction (PTTD)—now renamed progressive collapsing foot deformity (PCFD) to reflect that ligamentous structures beyond just the tendon contribute to the problem.
The Walking Debate: When Movement Helps and When It Hurts
Here’s the thing though—the relationship between walking and posterior tibial tendonitis isn’t black and white.
Complete rest sounds appealing when pain strikes. But prolonged immobilization creates its own problems: muscle atrophy, joint stiffness, and delayed return to normal function.
Protection and Relative Rest
Protection and relative rest are advised immediately after injury or during acute flare-ups, typically for the first 24 to 72 hours. During this window, reducing weight-bearing activities allows initial inflammation to settle.
That said, relative rest differs from complete bed rest. The goal is modifying activities rather than eliminating movement entirely.
Walking with posterior tibial tendonitis becomes acceptable once acute symptoms subside—provided proper precautions are in place. The tendon needs controlled loading to maintain strength and stimulate healing, but excessive stress interferes with tissue repair.
Pain as Your Guide
Pain level serves as the most reliable indicator for activity tolerance. Mild discomfort during walking that doesn’t worsen throughout the day or linger afterward suggests acceptable activity levels.
Sharp pain, significant limping, or symptoms that intensify with each step signal the need to reduce activity immediately. Swelling that increases during or after walking indicates excessive load.
The rule of thumb: if symptoms remain at baseline or improve within 24 hours of walking, the activity level is appropriate. Worsening symptoms mean scaling back.
Surface and Distance Matter
Not all walking creates equal tendon stress. Flat, even surfaces like sidewalks or tracks generate less strain than uneven terrain. Hills—particularly downhill walking—dramatically increase eccentric loading on the posterior tibial tendon.
Distance and duration require careful monitoring. Short walks may be tolerable when longer distances trigger symptoms. Gradually increasing distance as tolerance improves follows sound rehabilitation principles.
Treatment Strategies That Support Safe Walking
Walking with posterior tibial tendonitis becomes far more feasible when combined with appropriate treatment interventions. These strategies reduce tendon stress and support healing.
Footwear and Orthotic Support
Proper footwear dramatically impacts tendon loading. Shoes with firm heel counters, adequate arch support, and minimal heel-to-toe drop help control excessive foot pronation—the inward rolling motion that overstresses the posterior tibial tendon.
Custom or over-the-counter orthotic devices provide additional arch support, redistributing pressure away from the compromised tendon. In clinical studies examining non-surgical treatment, participants wore foot orthoses throughout the 12-week intervention for a minimum of 80% of weight-bearing tasks.
The orthotic doesn’t cure the condition but reduces mechanical stress during the healing phase, enabling continued activity within safe parameters.
Ice Application Protocol
Ice therapy helps manage pain and swelling. Apply cold packs to the most painful area of the posterior tibial tendon for 20 minutes at a time, 3 or 4 times a day.
Never apply ice directly to skin—use a thin towel or cloth barrier to prevent cold injury. Timing ice application after walking activity helps blunt the inflammatory response to mechanical loading.
Bracing Options
Ankle braces or walking boots may be recommended during acute phases or for patients with more advanced dysfunction. These devices limit excessive motion that stresses the tendon while permitting continued weight-bearing.
The specific device depends on condition severity. Simple ankle sleeves provide mild compression and proprioceptive feedback. Lace-up ankle stabilizers offer more substantial support. Controlled ankle motion (CAM) boots restrict motion significantly, used for severe cases or during specific healing phases.
| Support Level | Device Type | When Used | Walking Permitted |
|---|---|---|---|
| Minimal | Compression sleeve | Mild symptoms, maintenance phase | Yes, normal activity |
| Moderate | Lace-up brace with medial support | Active inflammation, Stage 1-2 | Yes, with modifications |
| Maximum | CAM boot or walking cast | Severe pain, Stage 2-3, post-surgery | Limited, short distances only |
| Surgical | Non-weight-bearing cast | Post-surgical recovery, severe rupture | No, crutches required |
Weight Management
Weight loss is a particularly effective way to reduce stress on the arch and its supporting structures. Given that obesity represents a significant risk factor—with more than 80% of PCFD patients carrying excess weight—losing even modest amounts reduces tendon loading during walking.
Every pound of body weight translates to multiple pounds of force through the foot during gait. Reducing weight directly decreases mechanical stress on the posterior tibial tendon with every step.
Rehabilitation Exercises: The Foundation of Recovery
Exercise plays a central role in posterior tibial tendonitis recovery. But timing and exercise selection matter enormously.
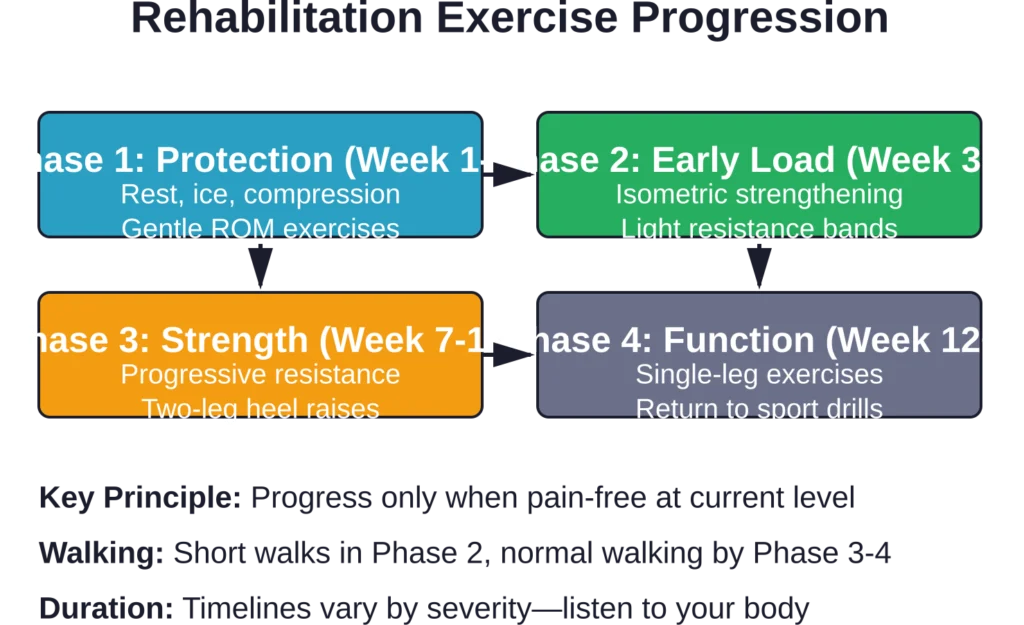
Early Phase Exercises
During the initial healing phase, gentle range-of-motion exercises maintain ankle mobility without overstressing the injured tendon. Ankle alphabet exercises—tracing letters with the foot—promote movement through multiple planes while keeping resistance minimal.
Isometric strengthening, where the muscle contracts without joint movement, allows early strength work without excessive tendon strain. Pressing the foot against an immovable surface activates the posterior tibial muscle while limiting tissue stress.
Common Exercise Mistakes
Real talk: certain exercises that seem logical actually flare up posterior tibial tendonitis in many patients.
Aggressive stretching where toes move closer to the shin (dorsiflexion stretches) frequently irritates the tendon during acute phases. The posterior tibial tendon experiences increased tension in this position, and forcing the stretch aggravates inflammation.
Practitioners treating this type of injury often find that patients flare themselves up with overly aggressive stretching early in recovery. If symptoms have persisted for an extended period and gentle stretches are attempted, caution remains essential.
Progressive Strengthening
As acute symptoms resolve, progressive resistance exercises rebuild tendon and muscle capacity. This phase typically begins 3-5 days per week to maintain strength and range of motion in the foot and ankle.
Resistance band exercises targeting foot inversion—turning the sole inward—directly strengthen the posterior tibial muscle. Starting with light resistance and gradually increasing load follows the principle of progressive overload necessary for tissue adaptation.
Single-leg balance exercises improve proprioception and functional strength. Standing on the affected leg for increasing durations, eventually progressing to unstable surfaces, rebuilds the neuromuscular control essential for normal walking mechanics.
Heel raises, starting with both feet and progressing to single-leg variations, represent the gold standard for posterior tibial strengthening. Beginning with partial range of motion and gradually increasing height challenges the tendon progressively.
The Warm-Up Rule
Before exercises or walking, a proper warm-up prepares tissues for activity. Low-impact options like stationary cycling or gentle walking for 5–10 minutes increase blood flow and tissue temperature, reducing injury risk.
Cold tissues are more prone to strain. The warm-up doesn’t need to be elaborate—just enough movement to transition from rest to activity gradually.
Activities to Avoid During Recovery
Certain activities create excessive posterior tibial tendon stress and should be modified or avoided during healing.
High-Impact Exercise
Running, jumping, and plyometric activities generate force magnitudes far exceeding walking. The repetitive impact loading overwhelms healing tissue capacity in most cases.
These activities typically need to be paused until significant strength returns and symptoms resolve. Attempting to run through posterior tibial tendonitis frequently extends recovery time substantially.
Cycling Considerations
Riding a bike with posterior tibial tendonitis produces mixed results. The foot position on the pedal places the ankle in dorsiflexion—toes elevated relative to the heel—which can irritate the tendon in some individuals.
That said, cycling doesn’t affect everyone with posterior tibial tendonitis equally. Some patients tolerate cycling well, while others experience symptom aggravation. Trial and error, guided by pain response, determines individual tolerance.
Barefoot Walking
Walking barefoot eliminates the arch support and shock absorption provided by proper footwear. For most patients with posterior tibial tendonitis, barefoot walking on hard surfaces increases symptoms.
At home, supportive sandals or slippers with arch support prove better than going completely barefoot. The tendon benefits from consistent support throughout the day, not just during exercise or outdoor walking.
Recovery Timeline: What to Expect
Recovery timelines vary depending on severity and treatment compliance. Conservative treatment is effective for most cases when caught early. Recovery may take weeks to months, with some cases requiring 6 months or more before significant improvement.
The 12-week intervention duration appears frequently in rehabilitation protocols, with significant improvements expected by this timeframe when treatment is appropriate and followed consistently.
But wait—recovery isn’t linear. Setbacks happen. A day when symptoms feel worse doesn’t mean treatment is failing. Gradual improvement over weeks and months, rather than day-to-day changes, provides the more reliable progress indicator.
Return to Normal Activity
Returning to full activity requires meeting specific criteria. Pain should be absent or minimal during daily activities. Single-leg heel raises should be possible without significant pain or weakness compared to the unaffected side.
Swelling should be minimal or absent after normal activity. The ability to walk for extended periods without symptom flare-up indicates readiness for more demanding activities.
Rushing return to activity increases re-injury risk substantially. Conservative progression, though frustrating, yields better long-term outcomes.
When Walking Becomes Problematic: Red Flags
Certain warning signs indicate walking should be reduced or medical evaluation sought.
Sharp, severe pain during walking suggests possible tendon tear rather than simple tendonitis. Sudden inability to perform a single-leg heel raise when previously possible warrants immediate evaluation.
Progressive arch collapse—the foot appearing flatter than before—indicates deteriorating tendon function. Numbness, tingling, or color changes in the foot suggest potential complications beyond tendonitis.
Symptoms persisting beyond 3 months despite appropriate conservative treatment warrant reassessment. Advanced imaging or specialist consultation may be necessary to rule out other pathology or assess for surgical candidacy.
Conservative vs. Surgical Treatment
Most posterior tibial tendonitis cases respond to conservative treatment when caught early. The combination of activity modification, orthotic support, exercise rehabilitation, and anti-inflammatory measures resolves symptoms in the majority of patients.
Surgery becomes consideration for patients who fail to improve after 6-12 months of appropriate conservative management or those with advanced tendon degeneration or rupture. Surgical options range from tendon debridement and repair to more extensive reconstructive procedures for severe deformity.
The specific procedure depends on condition stage and severity. Recovery from surgery typically requires 6-12 months, with protected weight-bearing and extensive rehabilitation.
| Treatment Phase | Primary Focus | Walking Status | Typical Duration |
|---|---|---|---|
| Acute | Reduce inflammation and pain | Limited, short distances only | 1-2 weeks |
| Subacute | Restore mobility and begin strengthening | Moderate walking with support | 3-6 weeks |
| Rehabilitation | Progressive strengthening and function | Normal walking distances | 6-12 weeks |
| Maintenance | Prevent recurrence, optimize biomechanics | Full activity with precautions | Ongoing |
Practical Walking Guidelines for Posterior Tibial Tendonitis
For those managing posterior tibial tendonitis while maintaining walking activity, these practical guidelines help balance activity with healing.
Start with short walks and gradually increase duration as tolerance permits. Walk on flat, even surfaces initially before progressing to varied terrain. Wear supportive footwear with orthotics for every walking session.
Monitor symptoms during and after walking. Mild discomfort is acceptable; sharp pain or significant limping indicates excessive load. Ice the tendon after longer walks to manage inflammation.
Incorporating rest days into the walking schedule. Alternating activity with rest periods allows tissue recovery between sessions.
Consider walking speed. Slower walking generates less force through the tendon than brisk walking. As strength improves, gradually increase pace.
Track symptoms in a simple log. Recording walking duration, pain levels, and next-day symptoms helps identify patterns and optimal activity dosing.
The Role of Professional Guidance
Working with healthcare professionals optimizes posterior tibial tendonitis management. Physical therapists assess biomechanics, prescribe individualized exercise programs, and employ manual therapy techniques addressing tissue restrictions.
Podiatrists evaluate foot structure and mechanics, prescribe custom orthotics, and recommend appropriate footwear modifications. Orthopedic specialists determine whether conservative treatment is appropriate or if surgical intervention should be considered.
Self-management plays an important role, but professional guidance increases treatment success rates and reduces the risk of progression to more severe dysfunction.
Long-Term Management and Prevention
Successfully recovering from posterior tibial tendonitis doesn’t mean the condition can’t recur. Long-term management focuses on addressing underlying risk factors and maintaining tendon health.
Continued use of supportive footwear and orthotics, even after symptoms resolve, helps prevent recurrence. Maintaining appropriate body weight reduces ongoing mechanical stress. Regular strengthening exercises preserve the muscle and tendon capacity developed during rehabilitation.
Addressing biomechanical issues that contributed to initial injury—whether through footwear, orthotics, or technique modification—forms the foundation of prevention.
For athletes or active individuals, cross-training reduces repetitive stress on the posterior tibial tendon. Alternating impact activities with low-impact options like swimming or cycling distributes load across different tissues.
Frequently Asked Questions
Initial rest for 24-72 hours helps reduce acute inflammation, but complete immobilization isn’t typically necessary beyond this period. After the initial phase, relative rest—reducing but not eliminating activity—combined with protective measures like orthotics and supportive footwear allows continued function while healing progresses. Most patients benefit from modifying rather than completely stopping activity.
Yes, excessive walking or walking without proper support can worsen posterior tibial tendonitis. Walking that causes sharp pain, significant limping, or symptoms that persist or worsen the next day indicates excessive load. However, appropriate walking with supportive footwear, orthotics, and appropriate distance typically doesn’t impede healing and may support recovery by maintaining tissue strength.
Shoes with firm heel counters, substantial arch support, minimal heel-to-toe drop, and good motion control work best for posterior tibial tendonitis. Avoid flat, flexible shoes, high heels, or minimalist footwear. Stability or motion control running shoes, even for walking, often provide appropriate support. Many patients benefit from adding custom or over-the-counter orthotic inserts for additional arch support.
Aggressive stretching, particularly dorsiflexion stretches where toes move toward the shin, often irritates the posterior tibial tendon during acute phases. If stretching is attempted after symptoms have been present for some time, only very gentle stretching should be used, and it should be discontinued if pain increases. Focus instead on strengthening exercises during the recovery phase.
Signs of healing include gradually decreasing pain levels, reduced swelling along the tendon, increasing ability to walk longer distances without symptom flare-up, and improving strength on single-leg heel raises. Progress typically occurs over weeks and months rather than day-to-day. Some fluctuation in symptoms is normal, but the overall trend should show improvement with appropriate treatment.
Mild cases occasionally resolve with simple rest, but most posterior tibial tendonitis cases require active treatment to heal properly and prevent progression. Without addressing the underlying biomechanical issues—typically excessive foot pronation and inadequate arch support—symptoms often persist or recur. Untreated posterior tibial tendonitis can progress to posterior tibial tendon dysfunction with permanent arch collapse.
Seek medical evaluation if symptoms persist beyond 2-3 weeks despite rest and home treatment, if pain is severe or prevents normal walking, if sudden inability to perform a single-leg heel raise occurs, if progressive arch flattening is noticed, or if numbness, tingling, or foot color changes develop. Early professional intervention improves treatment outcomes and prevents progression to more severe dysfunction.
Conclusion: Finding the Right Balance
So, is it okay to walk with posterior tibial tendonitis? The answer is nuanced.
Walking isn’t categorically prohibited, but it requires careful management. Appropriate support through footwear and orthotics, limited duration and intensity during acute phases, attention to pain signals, and progressive return to normal activity form the foundation of successful management.
Complete rest rarely serves as the optimal approach. Relative rest combined with targeted rehabilitation, biomechanical correction, and gradual return to function yields better outcomes than either extreme of continued high activity or complete immobilization.
The condition demands patience. Recovery takes weeks to months, not days. Rushing the process increases risk of progression to more severe, potentially permanent dysfunction.
If struggling with posterior tibial tendonitis, consult a physical therapist or podiatrist for individualized assessment and treatment planning. Professional guidance optimizes recovery and helps navigate the balance between rest and activity.
Walking with posterior tibial tendonitis is possible—with the right precautions, support, and rehabilitation approach guiding the journey back to pain-free function.