
Quick Summary: If a bee stinger remains lodged in the skin, it continues pumping venom for up to a minute, increasing pain, swelling, and risk of allergic reactions. While the body may eventually push out small stingers or absorb them, prompt removal within 30 seconds minimizes venom exposure and complications. Retained stingers can cause infection, prolonged inflammation, or in rare cases, serious systemic reactions requiring medical attention.
Getting stung by a bee is painful enough. But what happens when you can’t remove the stinger right away?
The short answer? That tiny barbed needle keeps working against you. Understanding what occurs when a stinger remains embedded helps explain why quick removal matters so much—and what to expect if extraction doesn’t happen immediately.
Why Bee Stingers Keep Delivering Venom After the Bee Leaves
Honey bees have a uniquely designed venom delivery system. According to medical research from the NIH, the stinger contains a venom sac with a piston-containing bifurcated stinger that can remain active even after separating from the bee’s body.
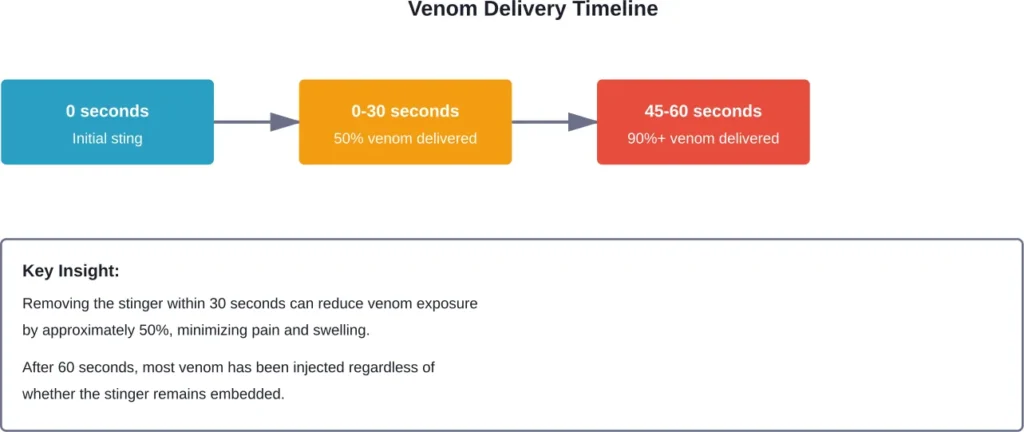
Here’s the thing though—when a honey bee stings, the barbed stinger lodges in your skin and tears away from the bee. The venom sac attached to that stinger continues contracting rhythmically, pumping venom into the wound for up to 60 seconds after the initial sting.
This means every second the stinger stays in place increases your venom exposure. The venom contains several active compounds including melittin, a hemolytic factor that causes cellular injury and pain.
What Actually Happens When a Stinger Stays In Your Skin
So you can’t get the stinger out immediately. What now?
According to MedicineNet, a bee stinger must be removed as a priority because it can cause serious consequences if not removed promptly. But the reality is more nuanced than that statement suggests.
Immediate Effects (First Few Hours)
The initial reaction to a retained stinger includes:
- Continued venom delivery for up to one minute
- Localized pain that intensifies around the sting site
- Redness spreading from the puncture point
- Swelling that develops within minutes
- Itching as histamine responses activate
Most people experience what doctors call a “local reaction.” The swelling typically remains confined to the sting area—maybe a 2-4 inch diameter around the puncture site. This is normal and doesn’t indicate an allergic reaction.
What Happens Over 24-48 Hours
If the stinger remains embedded past the first hour, several things occur:
The venom has already been fully injected, so the stinger itself becomes the primary concern. The chitinous exoskeleton of the stinger is relatively inert, according to medical commentary published in the Indian Journal of Ophthalmology. Some medical literature reports that stingers may be left in place without inciting further inflammation or may be spontaneously absorbed over time.
That said, most cases don’t resolve that smoothly.
Swelling often peaks 24-48 hours after the sting. If the stinger remains in place, this swelling can be more pronounced because the foreign body triggers ongoing immune responses. The area may feel warm to the touch as blood flow increases.
Infection Risk
A retained stinger creates a pathway for bacteria to enter beneath the skin surface. While not inevitable, infection becomes more likely if:
- The stinger remains embedded for more than 24 hours
- The area is scratched or irritated
- Proper wound cleaning didn’t occur
- The person has compromised immunity
Signs of infection include increasing pain after the first day, pus or discharge, red streaks extending from the sting site, and fever.
Can Your Body Eventually Expel or Absorb a Stinger?
Real talk: sometimes the body does handle this on its own.
The skin naturally pushes foreign objects toward the surface through a process involving immune cells and tissue regeneration. Small bee stingers may work their way out over several days to a week.
Alternatively, the immune system may encapsulate and break down the stinger material. Medical case reports document instances where stingers were left in place—particularly in eye injuries where surgical removal posed risks—and the chitinous material was eventually absorbed without major complications.
But this is the exception, not the rule. Relying on natural expulsion means accepting prolonged inflammation, higher infection risk, and extended discomfort.
When a Retained Stinger Becomes a Medical Emergency
According to the Texas A&M Honey Bee Lab, seek medical help immediately if breathing becomes difficult, the person was stung many times, or there’s a known allergy to bee stings.
Anaphylactic shock occurs relatively quickly and represents the most severe allergic response. According to medical authorities, quickly reaching medical help can save a life in cases of anaphylactic shock.
| Symptom Category | Normal Reaction | Emergency Signs |
|---|---|---|
| Swelling | Localized to sting area | Spreads beyond sting site, involves face or neck |
| Breathing | Normal | Difficulty breathing, wheezing, throat tightness |
| Skin | Redness at sting site | Hives across body, widespread flushing |
| Cardiovascular | Normal pulse | Rapid pulse, dizziness, fainting |
| Digestive | No symptoms | Nausea, vomiting, abdominal cramping |
A Cochrane systematic review confirmed that venom immunotherapy (VIT) is an effective treatment, reducing risk of a further systemic reaction (relative risk 0.10, 95% confidence interval 0.03–0.28).
Special Cases: When Stingers Get Stuck in Sensitive Areas
Location matters significantly when it comes to retained stingers.
Eye Injuries
Multiple case reports from NIH document serious complications from corneal bee stings. A recent review of literature reported that most cases of bee sting injuries underwent surgical removal of the stingers, with approximately 40% of cases with stinger removal showing clinical exacerbation post extraction. Retained stingers in the eye can cause:
- Corneal endothelial cell damage
- Secondary corneal abrasion
- Chronic keratouveitis
- Bullous keratopathy in severe cases
One documented case involved a beekeeper stung in the eyelid where the stinger migrated from the tarsal area onto the ocular surface over time, causing ongoing complications.
Multiple Stings
According to NIH research on bee sting complications, the greater the number of stings, the worse the prognosis because multiple stings lead to inoculation of higher amounts of venom. It is estimated that the lethality rate is about 0.29%, with an annual rate average incidence of 6.89 per 100,000 inhabitants.
Complications from multiple stings include acute kidney injury, cardiovascular effects, and systemic toxicity independent of allergic reactions.
What To Do If You Absolutely Cannot Remove the Stinger
Sometimes extraction isn’t immediately possible. Maybe the stinger broke off flush with the skin, or it’s in a location that’s difficult to reach.
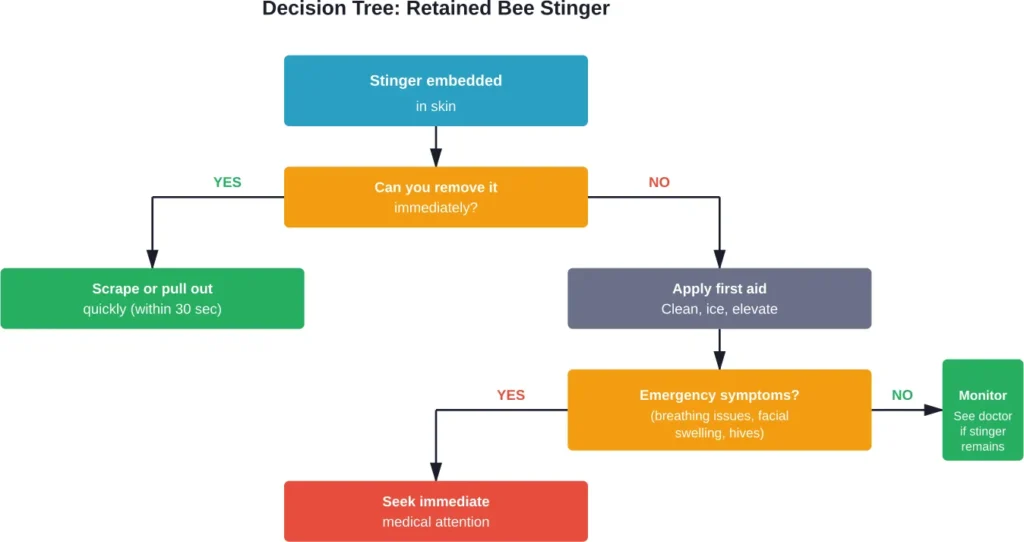
According to Cleveland Clinic Health Essentials, whether you scrape or pull out the stinger, the key is to do it quickly. But when that’s not feasible:
First aid steps:
- Clean the area thoroughly with soap and water
- Apply a cold pack for 10-15 minutes to reduce swelling and limit pain
- Elevate the affected area if possible
- Take an over-the-counter antihistamine to reduce itching
- Monitor for signs of infection or allergic reaction
Reapply the cold pack after waiting 10 minutes if pain persists.
If the stinger remains embedded after 24 hours, medical evaluation becomes advisable. Healthcare providers have specialized tools for extraction that minimize tissue damage.
Prevention: Reducing Risk of Future Stings
Prevent tetanus by staying up to date with vaccinations and seeking appropriate care after wounds. While tetanus from bee stings is rare, the wound created provides a potential entry point for Clostridium tetani spores common in soil and dust.
For those at high risk of stings (beekeepers, outdoor workers), wearing protective clothing makes sense. And for individuals with known severe allergies, carrying an epinephrine auto-injector is essential.
Data from medical research shows that venom immunotherapy dramatically reduces future reaction risks. For people who’ve experienced systemic allergic reactions, this treatment can be life-changing.
The Tetanus Connection Nobody Talks About
Here’s something that doesn’t get mentioned enough: any puncture wound carries tetanus risk.
According to the CDC, tetanus spores from the environment enter the body through cuts or wounds. The bacteria don’t spread person to person, but they’re ubiquitous in soil, dust, and manure.
If you haven’t had a tetanus booster in the past five years and you’re stung, especially if the stinger creates a deep puncture, a tetanus shot may be warranted. This is particularly true if the sting occurred outdoors in an environment where tetanus spores are common.
Myths About Stinger Removal Methods
A systematic review published in Cureus examined various bee stinger removal methods. Community discussions often debate whether scraping versus pulling makes a difference.
The research conclusion? Speed matters more than method. Whether you scrape with a credit card edge or pull with tweezers, removing the stinger within 30 seconds provides the greatest benefit.
Some myths that persist:
- Myth: Squeezing releases more venom. Reality: The venom sac contracts automatically; carefully removing it quickly is better than waiting to find the “perfect” tool.
- Myth: You should leave the stinger in to avoid making it worse. Reality: Prompt removal always reduces venom exposure.
- Myth: Only allergic people need to worry about stingers. Reality: Anyone can develop infections or complications from retained foreign bodies.
Long-Term Outlook and Complications
For most people, even a retained stinger resolves without lasting effects. The body’s immune system eventually handles the foreign material, inflammation subsides, and healing occurs.
But medical literature documents rare serious complications. Case reports include cardiac effects weeks after multiple stings, kidney injury from mass envenomation, and chronic inflammatory responses.
One documented case involved a patient who developed a prolonged heart block, syncope, and cardiac arrest approximately three weeks after multiple bee stings, requiring permanent pacemaker implantation.
These severe outcomes remain exceptional, with most cases resolving without complications.
Frequently Asked Questions
A stinger can technically remain embedded for days or weeks, though this isn’t advisable. The venom delivery completes within 60 seconds, but the foreign body can cause ongoing inflammation, infection risk, and discomfort until removed or naturally expelled.
Sometimes the body naturally pushes a stinger toward the skin surface over several days. Medical literature documents cases where small stingers were absorbed by the immune system. However, relying on natural expulsion means accepting higher complication risks and prolonged symptoms.
If you can’t locate a stinger visually, it may have already fallen out, broken off flush with the skin, or never fully embedded. Clean the area thoroughly, apply ice, and monitor for infection signs. If swelling worsens after 24 hours or you develop fever, see a healthcare provider.
Yes, any foreign body that penetrates the skin creates infection risk. Bacteria can enter through the puncture site, especially if the area is scratched or not properly cleaned. Signs of infection include increasing pain after the first day, pus, red streaks, and fever.
Seek immediate medical attention if you experience difficulty breathing, facial or throat swelling, hives across your body, rapid pulse, dizziness, or nausea. Also see a doctor if a stinger cannot be removed after 24 hours, if infection signs develop, or if you haven’t had a tetanus booster in five years.
According to systematic medical review, speed of removal matters more than technique. Whether you scrape with a card edge or pull with tweezers, removing the stinger within 30 seconds minimizes venom exposure. Don’t waste time searching for the “perfect” tool—use whatever is available quickly.
Multiple bee stings delivering large amounts of venom can cause acute kidney injury according to NIH research. This typically requires dozens to hundreds of stings. Single stings rarely cause systemic organ damage in people without severe allergies, though documented cases exist of complications from mass envenomation events.
Final Thoughts
Look, most bee sting situations resolve without drama. Even if the stinger stays in for a few hours, you’ll probably be fine with proper wound care and monitoring.
But the science is clear: quick removal within 30 seconds reduces venom exposure and minimizes your reaction. When that’s not possible, thorough cleaning, cold compression, and vigilant monitoring become your best tools.
Watch for the red flags—breathing difficulty, spreading swelling, signs of infection. Those require professional medical attention, not home remedies.
And if you’ve experienced a severe reaction to a sting before? Don’t take chances. Carry epinephrine, avoid known sting risks, and talk to an allergist about venom immunotherapy. The data shows it works.
Stay safe out there. And keep those tweezers handy.