
Quick Summary: Getting semen in the eye causes temporary irritation (stinging, redness, blurry vision) that typically resolves within 24 hours. Rinse immediately with water or saline solution without rubbing. While STI transmission through ocular contact is rare, it’s possible with infections like chlamydia and gonorrhea—follow up with testing if exposure occurred with a partner of unknown status.
Things don’t always go according to plan during intimate moments. One minute everything’s going fine, and the next, semen lands directly in the eye. It happens more often than most people realize, and whether intentional or accidental, the immediate reaction is usually panic.
The good news? This situation is manageable with the right information. Understanding what happens physiologically, knowing the immediate steps to take, and recognizing when medical attention becomes necessary can prevent complications and reduce anxiety about potential health risks.
This guide covers everything from immediate care to long-term considerations around sexually transmitted infections.
Immediate Response: What to Do Right Now
Speed matters when semen gets in the eye. The faster the response, the less irritation and lower the risk of complications.
Don’t Rub—Rinse Instead
The instinctive reaction is to rub the affected eye. Resist this urge completely. Rubbing pushes irritants deeper into eye tissue and can cause corneal abrasions, especially if semen contains bacteria or viral particles.
Instead, rinse immediately with clean water or saline solution. Hold the eye open under a gentle stream of lukewarm water for at least 60 seconds. Alternatively, fill a clean bowl with water or saline and submerge the eye while blinking repeatedly to flush out the semen.
Contact lens wearers should keep lenses in during the initial rinse, then remove and thoroughly clean or discard them afterward. Removing lenses first can trap semen between the lens and cornea.
Keep Flushing
One rinse usually isn’t enough. Continue flushing the eye with water or over-the-counter eye drops every few hours for the first day. This dilutes remaining proteins and acids that cause irritation.
Sterile saline solution works better than tap water, but any clean water source is acceptable in the immediate aftermath when saline isn’t available.
What Causes the Burning and Irritation
Semen is a complex bodily fluid containing proteins, enzymes, zinc, fructose, and various acids. The eye’s delicate tissues react strongly to these foreign substances.
The burning sensation comes primarily from the acidic pH of semen interacting with the eye’s neutral environment. Enzymes present in seminal fluid can irritate the conjunctiva (the membrane covering the white part of the eye) and cornea.
Zinc concentrations in semen are particularly high—higher than in most other body tissues. While zinc itself isn’t harmful, concentrated exposure causes a stinging reaction in sensitive eye tissue.
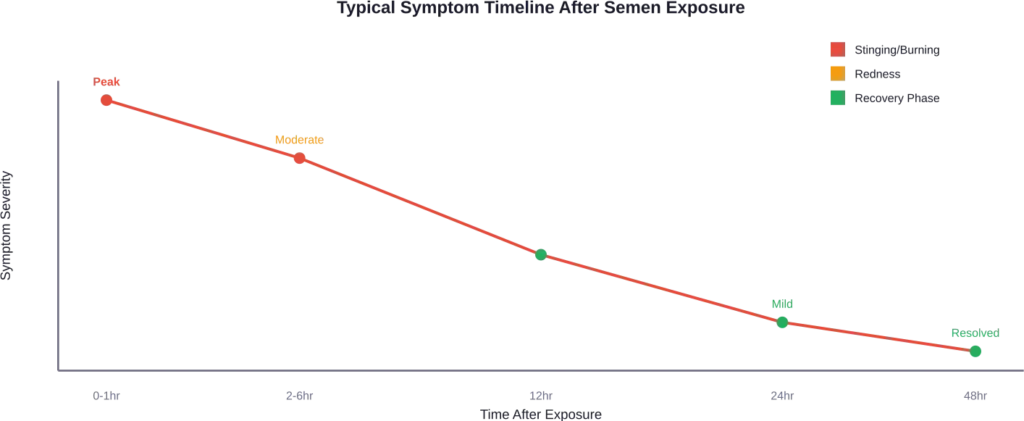
Common Symptoms and Duration
Expect several predictable symptoms after semen exposure to the eye. Understanding what’s normal versus what requires medical attention helps avoid unnecessary panic.
Stinging and Burning
Intense stinging begins immediately upon contact. This sensation typically peaks within 5-10 minutes and gradually decreases over the next few hours. The burn should be noticeably better within 2-3 hours of thorough rinsing.
Persistent or worsening burning beyond 6 hours suggests incomplete flushing or possible infection.
Redness and Bloodshot Appearance
The eye turns red as blood vessels in the conjunctiva dilate in response to irritation. This inflammatory response is protective, bringing immune cells to the affected area.
Redness usually develops within 30 minutes and can last up to 24 hours. Some residual pinkness may persist for 48 hours. If redness intensifies after the first day rather than fading, medical evaluation becomes necessary.
Blurry Vision
Temporary blurriness results from tear production and protein deposits on the corneal surface. Vision typically clears within 1-4 hours as natural tears wash away residue.
Blurry vision lasting beyond 6 hours or progressive vision loss requires immediate medical attention.
Watering and Discharge
Excessive tearing is the eye’s natural defense mechanism. Increased tear production helps dilute and flush out foreign substances. This symptom should decrease significantly within 2-3 hours.
Clear discharge is normal. Yellow or green discharge indicates possible bacterial infection and requires medical evaluation.
Relief Measures That Actually Help
Several strategies can reduce discomfort during the recovery period.
Cool or warm compresses provide immediate relief. Dampen a clean washcloth with cool water for acute burning or warm water for general discomfort. Apply gently to the closed eye for 5-10 minutes every few hours.
Over-the-counter pain relievers like ibuprofen or acetaminophen reduce inflammation and discomfort. Standard dosing is sufficient—no need for maximum doses.
Artificial tears or lubricating eye drops soothe irritation and continue flushing residual proteins. Use preservative-free formulations to avoid additional irritation. Apply drops every 1-2 hours for the first day.
Avoid touching or rubbing the eye, even when itching develops. Keep hands away from the face entirely if possible.
Understanding STI Transmission Risks
The question that causes the most anxiety: can sexually transmitted infections spread through semen contact with the eye?
Yes, but transmission rates are significantly lower than genital exposure. The eye lacks the warm, moist environment that most STI pathogens prefer, and tear film contains antimicrobial properties that provide some protection.
That said, certain infections can and do transmit through ocular exposure.
Chlamydia and the Eye
Chlamydia trachomatis is the most frequently reported bacterial infectious disease in the United States, with prevalence highest among persons aged ≤24 years. The pathogen can cause conjunctivitis (pink eye) when introduced to ocular tissues.
Research published in medical literature documents cases where direct ejaculation into the eye resulted in chlamydial conjunctivitis. Symptoms typically develop within 5-14 days of exposure and include persistent redness, discharge, and discomfort that doesn’t resolve like simple irritation.
Without treatment, chlamydial eye infections can affect the cornea, potentially leading to keratitis. According to medical research, these complications may occur within 24 hours of infection and require prompt diagnosis.
Gonorrhea Transmission
Gonorrhea can transmit to the eye through semen contact, causing gonococcal conjunctivitis. This infection is more aggressive than chlamydial conjunctivitis and progresses faster.
Symptoms include severe redness, copious yellow-green discharge, swollen eyelids, and significant pain. Gonococcal eye infections can cause serious corneal damage within 24-48 hours without treatment.
Medical literature indicates gonorrhea transmission through direct ocular contact is possible, though less efficient than genital transmission.
HIV and Ocular Exposure
HIV transmission through semen in the eye is theoretically possible but extremely rare. A review examining documented occupational exposure cases estimated very low transmission risk through mucous membrane contact.
The CDC tracks occupational exposures to HIV-infected fluids. While the exact per-exposure risk for ocular contact hasn’t been definitively quantified, it’s considerably lower than risks associated with needle stick injuries or receptive anal/vaginal intercourse.
That said, post-exposure prophylaxis (PEP) may be recommended depending on the source partner’s HIV status and viral load. PEP must be initiated within 72 hours of exposure to be effective.
Herpes Simplex Virus
HSV-1 and HSV-2 can both cause ocular herpes, though HSV-1 is more commonly associated with eye infections. An estimated 3.8 billion people under age 50 (64%) globally have herpes simplex virus type 1 (HSV-1) infection.
Herpes eye infections present with pain, light sensitivity, watering, and sometimes visible sores on the eyelid. These infections can recur and potentially affect vision if corneal involvement develops.
Syphilis Considerations
Ocular syphilis can occur at any stage of syphilis infection. The CDC notes healthcare providers should screen patients for syphilis if they present with visual complaints and risk factors.
While transmission through a single exposure of semen to the eye is less documented than with chlamydia or gonorrhea, the possibility exists, especially with a partner who has active syphilis infection.

When to Seek Medical Attention
Most cases of semen in the eye resolve without medical intervention. However, certain symptoms warrant professional evaluation.
See a doctor or visit urgent care if:
- Redness intensifies after 24 hours rather than improving
- Pain worsens or becomes severe
- Vision changes persist beyond 6 hours or progressively worsen
- Yellow or green discharge develops
- Light sensitivity becomes extreme
- The eye feels like something is still in it despite thorough rinsing
- Symptoms haven’t improved at all after 48 hours
These signs may indicate infection rather than simple irritation.
Emergency evaluation is necessary for severe pain, sudden vision loss, or inability to open the eye due to swelling.
STI Testing Recommendations
Testing becomes important when the source partner’s STI status is unknown or when they’re known to have an infection.
When to Get Tested
If the exposure involved a partner whose STI status is uncertain or positive, schedule comprehensive STI screening. Even without symptoms, testing provides peace of mind and catches infections that may be asymptomatic initially.
For partners in monogamous relationships with recent negative testing and documented monogamy, additional screening may not be necessary unless symptoms develop.
Testing Timeline
Different infections have different window periods—the time between exposure and when tests can reliably detect infection.
| Infection | Recommended Testing Time | Notes |
|---|---|---|
| Chlamydia | 14 days post-exposure | Earlier testing possible if symptoms develop |
| Gonorrhea | 14 days post-exposure | Earlier testing possible if symptoms develop |
| HIV | 45-90 days for conclusive results | Earlier testing at 2-4 weeks can detect most cases |
| Syphilis | 6 weeks to 3 months | Repeat testing may be needed |
| Herpes | 4-6 weeks | Type-specific antibody testing |
Many sexual health clinics recommend baseline testing immediately, then follow-up testing at 2 weeks and 3 months to catch infections across different window periods.
Testing Process
Standard STI testing for ocular exposure is the same as testing for genital exposure—blood tests for HIV, syphilis, and herpes; urine tests or swabs for chlamydia and gonorrhea.
If eye symptoms develop that suggest infection, an ophthalmologist may take a conjunctival swab to identify the specific pathogen causing ocular symptoms.
Treatment Options
Treatment depends entirely on whether infection is present and which pathogen is identified.
For simple irritation without infection, no medical treatment is necessary beyond supportive care—rinsing, artificial tears, and time.
Doxycycline is effective for chlamydia treatment. For gonorrhea, treatment approaches vary; CDC guidelines note that a randomized trial reported 100% microbiologic cure with doxycycline for rectal chlamydia among MSM and 74% with azithromycin.
Ocular infections may require both systemic antibiotics (pills) and topical antibiotic eye drops or ointments to address the infection comprehensively.
Herpes eye infections are treated with antiviral medications, either oral antivirals like valacyclovir or topical antiviral eye preparations. Prompt treatment is essential to prevent corneal scarring.
For HIV exposure from a known positive source or high-risk situation, post-exposure prophylaxis involves a 28-day course of antiretroviral medications. This must begin within 72 hours of exposure, with earlier initiation being more effective.
Prevention Strategies
While accidents happen, several strategies reduce the likelihood of semen getting in the eye during sexual activity.
Communication with partners about preferred practices and boundaries helps both people understand what’s comfortable and what’s off-limits. Discussing facial ejaculation preferences before the moment arrives prevents misunderstandings.
During oral sex or other activities where ejaculation might occur near the face, closing eyes or turning the head provides simple physical protection.
Using barriers like condoms during oral sex eliminates the possibility of direct semen contact entirely. Flavored condoms are specifically designed for oral use.
For partners with known STIs, treatment and viral suppression reduce transmission risks substantially. Partners on effective HIV treatment with undetectable viral loads, for instance, cannot transmit HIV sexually (undetectable equals untransmittable).
Regular STI screening for all sexually active individuals creates awareness of infection status, allowing for informed decision-making and timely treatment.
Frequently Asked Questions
Blindness from semen exposure alone is extremely unlikely. The irritation caused by semen’s chemical composition doesn’t cause permanent damage. However, if semen transmits an untreated STI like gonorrhea or chlamydia that progresses to serious corneal infection, vision damage becomes possible without prompt medical treatment. This scenario is rare but emphasizes the importance of monitoring symptoms and seeking care if they worsen.
Typical irritation resolves within 24-48 hours. Stinging and burning peak in the first hour and should noticeably improve within 2-6 hours. Redness can persist for up to 48 hours. If symptoms haven’t improved after two days or worsen after the first day, medical evaluation is recommended to rule out infection.
No. Eye patches aren’t recommended for this type of exposure. Patches create a warm, moist environment that can promote bacterial growth if any pathogens are present. Keep the eye open, continue flushing periodically, and allow natural tears and blinking to continue the cleaning process. Only wear an eye patch if specifically instructed by a healthcare provider.
Wait until all symptoms completely resolve before wearing contacts again. If wearing contacts during exposure, remove and thoroughly clean them after the initial rinse, or better yet, discard daily lenses and use a fresh pair once symptoms clear. Never wear contacts while the eye is red, irritated, or producing discharge, as this can trap bacteria and worsen potential infections.
It depends on the partner’s status. If the partner’s STI status is unknown or they have a known infection, testing is recommended even without symptoms. Many STIs can be asymptomatic initially, and ocular infections specifically may take days to develop noticeable symptoms. Testing provides definitive answers and enables early treatment if needed. For monogamous partners with recent negative tests, additional screening may be unnecessary.
Chemical irritation from semen’s natural composition causes immediate symptoms (within minutes) that steadily improve over 24-48 hours. Infection symptoms typically appear days after exposure (3-14 days for most STIs) and progressively worsen rather than improve. Infection usually involves yellow or green discharge, whereas chemical irritation produces clear tears. Infections also tend to cause more severe pain, light sensitivity, and vision changes compared to simple irritation.
Immediate rinsing significantly reduces transmission risk by removing infectious material before pathogens can penetrate tissue or establish infection. However, it doesn’t guarantee prevention. Some pathogens work quickly, and the eye’s mucous membranes absorb substances rapidly. Rinsing is absolutely the right first step and likely prevents many infections, but follow-up testing remains important for high-risk exposures because rinsing isn’t 100% effective.
Moving Forward
Getting semen in the eye ranks among the more awkward sexual mishaps, but it’s also one of the most manageable. Immediate rinsing addresses the acute irritation, and awareness of STI transmission possibilities ensures appropriate follow-up.
Most cases resolve completely within a day or two without complications. The key is knowing when normal irritation crosses into potential infection territory and seeking medical care when symptoms suggest something beyond simple chemical irritation.
Regular STI testing, open communication with partners, and understanding transmission risks create the foundation for sexual health. These practices matter regardless of this specific situation—they’re fundamental to maintaining health in any sexual relationship.
If symptoms persist, worsen, or cause concern, don’t hesitate to consult a healthcare provider or ophthalmologist. Professional evaluation provides definitive answers and appropriate treatment when needed, protecting both immediate comfort and long-term eye health.