Quick Summary: Leaving ear drops in too long typically causes no harm for most over-the-counter formulations, as excess liquid naturally drains out. However, extended or improper use of certain prescription drops—particularly those containing ototoxic ingredients like aminoglycosides—can lead to complications including irritation, maceration of ear canal skin, or in rare cases with perforated eardrums, potential inner ear damage. Most ear drops should remain in the ear for 5-10 minutes maximum, and any concerns about duration or side effects warrant medical consultation.
The bottle says to leave the drops in for a few minutes. But what if you dozed off? Or got distracted and forgot about them for half an hour?
Here’s the thing—most people worry about this exact scenario. And the answer depends heavily on what type of ear drops you’re using and the condition of your eardrum.
Let’s break down what actually happens when ear drops overstay their welcome, the real risks involved, and when you should be concerned.
Understanding How Ear Drops Work
Ear drops are liquid medications designed to treat various ear conditions. Ear drops can help treat pain, inflammation, infection, and earwax blockage. The active ingredients vary dramatically based on the intended use.
The ear canal isn’t just a straight tube—it’s a curved passage lined with delicate skin that produces protective earwax. When drops enter this space, they need enough time to reach the affected area and work their magic. But there’s a natural drainage system at play too.
Most ear drops are designed to work within a specific timeframe. The liquid coats the ear canal, delivers medication to the target tissue, then gradually drains out through natural head movement and gravity. This is why instructions typically tell you to lie on your side for 5-10 minutes after application.
Types of Ear Drops and Their Active Ingredients
Not all ear drops carry the same risks when left in too long. The ingredients matter significantly.
| Ear Drop Type | Primary Use | Common Ingredients | Overuse Risk Level |
|---|---|---|---|
| Cerumenolytics | Earwax removal | Carbamide peroxide, mineral oil | Low to moderate |
| Antibiotic drops | Bacterial infections | Ciprofloxacin, ofloxacin, neomycin | Moderate to high |
| Anti-inflammatory | Reduce swelling | Hydrocortisone, dexamethasone | Moderate |
| Analgesic drops | Pain relief | Benzocaine, antipyrine | Low |
| Antifungal drops | Fungal infections | Clotrimazole, acetic acid | Low to moderate |
What Actually Happens When Drops Stay In Too Long
The immediate answer? Usually nothing dramatic.
For most over-the-counter ear drops used to soften earwax or relieve minor pain, leaving them in an extra 20-30 minutes won’t cause significant problems. The excess liquid simply drains out when you move your head.
But here’s where it gets more complicated.
Skin Irritation and Maceration
The ear canal skin is remarkably thin and sensitive. Prolonged exposure to liquid—any liquid—can cause maceration. This is the same wrinkling effect you see on your fingertips after a long bath, but inside your ear canal.
Extended contact with ear drops can lead to skin breakdown in the external auditory canal. The protective barrier weakens, making the area more vulnerable to infection.
Symptoms of this irritation include itching, redness, and a feeling of dampness that won’t resolve. The ear canal might feel raw or tender to touch.
Chemical Burns and pH Imbalance
Some ear drops contain ingredients with low pH levels or alcohol. According to AAO-HNS clinical practice guidelines, topical drops containing alcohol or low pH should be avoided if the tympanic membrane is non-intact because of pain and potential ototoxicity.
When these formulations sit in the ear canal for extended periods, they can cause chemical irritation. The natural pH balance of the ear canal (typically slightly acidic) gets disrupted. This creates an environment where harmful bacteria or fungi can thrive.
Real talk: if you’ve ever felt a burning sensation after using ear drops, that’s your body signaling the chemicals are too harsh or staying in contact too long.
The Ototoxicity Risk: When Ear Drops Become Dangerous
Now we’re getting to the serious stuff.
Ototoxicity refers to damage to the inner ear structures—particularly the cochlea and vestibular system—caused by medications or chemicals. An estimated 1.57 billion people globally had hearing loss in 2019, with ototoxic medications being one contributor among many causes.
Here’s what makes certain ear drops potentially dangerous when overused or left in too long.
Aminoglycoside Antibiotics: The Main Culprits
Neomycin, polymyxin, and similar aminoglycoside antibiotics are highly effective against bacteria. But they’re also known ototoxins. MedlinePlus drug information warns that these substances can cause permanent hearing loss when they reach the inner ear.
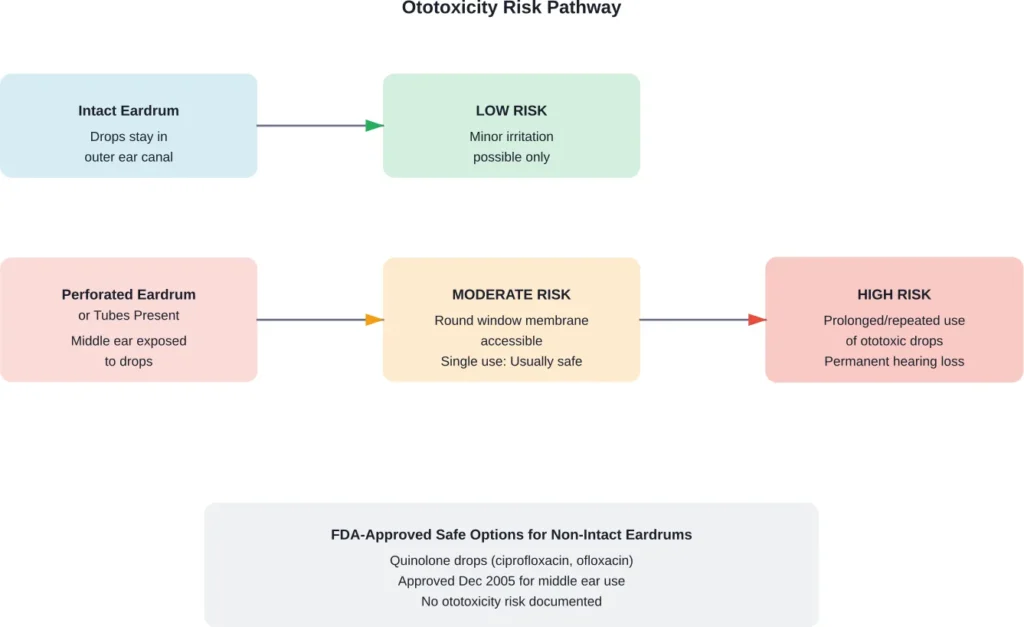
The catch? With an intact eardrum, these drops generally can’t reach the inner ear. They stay confined to the outer ear canal where they belong.
But if your eardrum is perforated—or if you have tympanostomy tubes—the middle ear space becomes open. The round window membrane, which separates the middle ear from the inner ear, becomes accessible. And that’s when ototoxic ingredients can potentially cause permanent damage.
According to the AAO-HNS clinical practice guidelines, severe hearing loss has been observed after prolonged or repetitive administration of topical ototoxic drops in patients with non-intact tympanic membranes. A single short course typically doesn’t cause problems, but extended use absolutely can.
The Inflammation Paradox
There’s an interesting clinical observation worth noting. During the initial treatment phase for acute otitis externa with a perforated eardrum, middle ear inflammation creates swelling that partially protects the round window membrane.
But as treatment progresses and inflammation decreases, the round window becomes more accessible. This means the inner ear actually becomes more vulnerable to ototoxic agents later in the treatment course.
So counterintuitively, extended use might be more dangerous than initial use—even if the first few applications seemed fine.
Specific Risks by Ear Drop Type
Carbamide Peroxide for Earwax
According to research, ten percent of children and five percent of the adult population experience earwax-related conditions.
Carbamide peroxide works by releasing oxygen, which helps break down earwax. But leaving it in too long can cause excessive bubbling, irritation, and dryness. A homemade ear drop alternative mentioned is a 15% baking soda solution., but similar duration limits apply.
The recommended contact time is typically 5-15 minutes. Going beyond this doesn’t improve effectiveness—it just increases irritation risk.
Antibiotic Ear Drops
Ciprofloxacin and ofloxacin (quinolone antibiotics) are FDA-approved for middle ear use without documented ototoxicity risk. These are considered safe even with perforated eardrums.
But older formulations containing neomycin come with explicit manufacturer warnings against use with non-intact tympanic membranes. The warning specifically cites the risk of permanent sensorineural hearing loss.
If symptoms don’t improve after one week of antibiotic ear drop use, medical consultation is necessary. Continuing beyond prescribed duration without medical guidance increases both resistance and complication risks.
Pain Relief Drops
Numbing analgesic ear drops typically start working within 15-30 minutes, producing a cooling sensation as pain relief begins. The numbing sensation signals they’re active.
These formulations carry lower risks when left in too long compared to antibiotics. The main concern is local allergic reactions or skin sensitivity with prolonged contact. Some individuals develop contact dermatitis from benzocaine specifically.
Signs Your Ear Drops Have Been In Too Long
How do you know if you’ve crossed the line from therapeutic to problematic?
Watch for these warning signs:
- Increased pain or burning sensation rather than relief
- Persistent drainage that continues hours after application
- New itching or feeling of rawness in the ear canal
- Dizziness or balance problems (suggests inner ear involvement)
- Changes in hearing quality or muffled sounds
- Tasting the medication in your throat (indicates perforation)
- Skin peeling or flaking visible at the ear canal entrance
That last symptom—tasting ear drops—is particularly important. If you can blow air out of your ear canal while pinching your nose, or if you taste medicine placed in your ear, you have a perforation. This changes the entire risk profile.
How Long Should Ear Drops Actually Stay In?
Let’s get specific with timeframes.
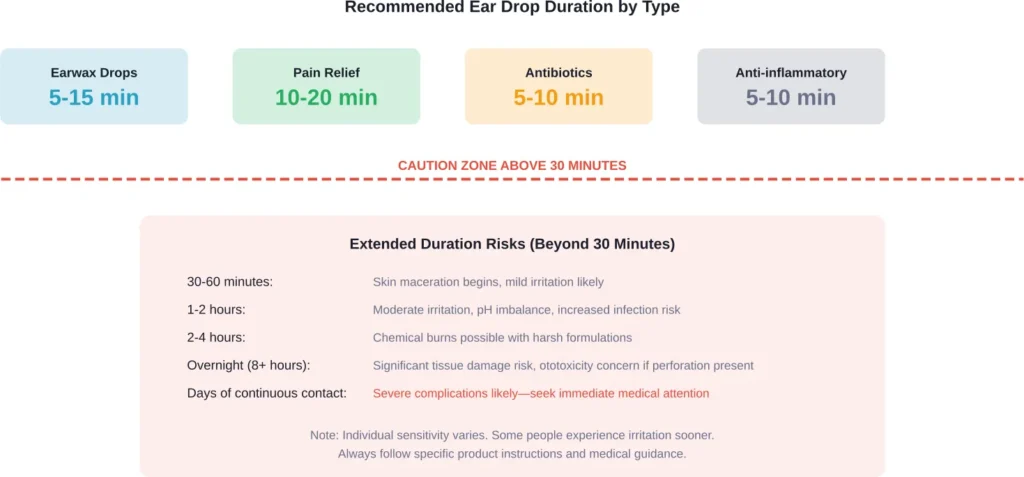
Most instructions specify lying on your side for 5-10 minutes after application. This allows the drops to coat the ear canal and reach the target area. After this window, sitting up and allowing excess to drain is appropriate.
The one-hour mark is where most medical professionals draw a cautionary line. Beyond this, you’re entering territory where side effects become more probable, especially with medicated formulations.
What to Do If You’ve Left Drops In Too Long
So you fell asleep with ear drops in. Now what?
First, don’t panic. The occasional extended application typically won’t cause permanent damage, especially with over-the-counter earwax softeners.
Here’s the action plan:
- Drain the excess immediately by tilting your head to the affected side
- Gently pull your earlobe in different directions to help drainage
- Use a clean tissue (never cotton swabs) to absorb liquid at the ear canal entrance
- Monitor for symptoms of irritation over the next 24-48 hours
- Discontinue use if burning, increased pain, or new symptoms develop
- Contact a healthcare provider if symptoms worsen or don’t resolve within 2-3 days
What you shouldn’t do: Don’t try to flush your ear with water or alcohol-based solutions. This can compound irritation. Don’t insert cotton swabs, bobby pins, or any objects to dry the canal—this risks further injury.
Preventing Complications: Best Practices
The best approach? Use ear drops correctly from the start.
Warm the bottle by holding it in your hand for 1-2 minutes before application. Cold drops can cause dizziness when they contact the eardrum. This recommendation appears consistently across medical guidelines.
Position matters tremendously. Lie on your side with the affected ear facing upward. Some people find placing a folded towel under their head maintains the angle more comfortably.
Set a timer. Seriously. Five minutes feels much longer than you think when you’re lying still. A timer prevents the “I’ll just rest my eyes” scenario that leads to extended contact time.
After the recommended duration, remain lying down for an additional 1-2 minutes, then sit up slowly. Tilt your head to allow drainage. Some liquid remaining in the canal is normal—it will work its way out naturally.
When Extended Use Is Medically Necessary
There’s a caveat to everything discussed so far.
Sometimes healthcare providers prescribe extended-duration ear drop protocols for specific conditions. For severe earwax impaction, multiple daily applications over several days might be necessary. For chronic ear infections, week-long antibiotic courses are standard.
The difference? Medical supervision and appropriate medication selection.
Cerumen impaction can occlude the external auditory canal or press against the tympanic membrane, potentially causing ear fullness, conductive hearing loss, itching, and pain. Treatment might require multiple interventions including repeated ear drop applications and professional irrigation. This is medically appropriate—but it’s not the same as accidentally leaving drops in too long.
If your healthcare provider prescribes a specific duration or frequency, that guidance supersedes general recommendations. The prescribing decision accounts for your specific ear anatomy, condition severity, and medication risks.
Special Populations at Higher Risk
Children
According to the research data, 10% of children experience earwax obstruction—double the rate in adults. Pediatric ear canals are smaller and more delicate.
Children also can’t reliably report subtle symptoms like mild burning or itching until it becomes severe. Seattle Children’s Hospital emphasizes careful monitoring for pain or bleeding after any ear canal manipulation.
For children, err on the side of shorter application times. Five minutes is sufficient for most pediatric ear drop formulations.
People with Ear Tubes
Tympanostomy tubes typically remain in place for varying durations depending on tube type and individual factors. During this entire period, the eardrum should be considered non-intact.
This completely changes which ear drops are safe. Only quinolone antibiotics (ciprofloxacin, ofloxacin) should be used. Neomycin-containing drops are explicitly contraindicated.
Duration is also more critical. The open pathway to the middle ear means ototoxic substances have direct access to the round window membrane. Even “safe” medications should only remain for the minimum effective time.
Individuals with Diabetes or Compromised Immunity
Diabetes and immunocompromised states increase the risk of malignant otitis externa—a severe, spreading infection of the ear canal and skull base. While rare, it’s life-threatening.
For these individuals, any ear drop complication that introduces bacteria into damaged tissue carries heightened risk. Strict adherence to duration guidelines and monitoring for worsening symptoms becomes even more important.
Frequently Asked Questions
For over-the-counter earwax drops with an intact eardrum, overnight exposure very rarely causes permanent hearing loss. However, prescription antibiotic drops containing aminoglycosides (like neomycin) can potentially cause permanent sensorineural hearing loss if you have a perforated eardrum or ear tubes and the drops remain in contact for extended periods. According to the AAO-HNS, severe hearing loss has been documented after prolonged or repetitive use of ototoxic drops in patients with non-intact tympanic membranes, though a single short course typically doesn’t cause permanent damage.
Key signs of eardrum perforation include tasting medication placed in your ear, being able to blow air out of your ear canal while pinching your nose closed, sudden sharp pain followed by relief, drainage of fluid or blood from the ear, or recent severe ear infection. If you have tympanostomy tubes, your eardrum should be considered non-intact for the entire time the tubes remain in place (typically 6-12 months minimum). If you’re unsure, a healthcare provider can examine your ear and determine eardrum status definitively.
Mild warmth or tingling is normal with some ear drops, especially those containing carbamide peroxide. But significant burning suggests irritation or an adverse reaction. Immediately tilt your head to drain the drops out. Use a clean tissue to absorb excess liquid at the ear canal entrance—never insert anything into the canal. If burning persists more than 10-15 minutes after removal, or if you develop increased pain, swelling, or discharge, contact your healthcare provider. Discontinue that product and bring the bottle to your medical appointment so the ingredients can be reviewed.
Not necessarily. Homemade solutions like mineral oil or saline may seem gentler, but they still carry risks with prolonged contact. Seattle Children’s Hospital mentions 15% baking soda solution as a homemade alternative for earwax softening, but the same duration guidelines apply—typically 5-15 minutes maximum. The advantage of commercial products is standardized pH, sterility, and tested formulations. Homemade solutions can vary in concentration and may harbor contaminants if not prepared properly. Whether homemade or commercial, prolonged contact with any liquid can cause skin maceration and increase infection risk.
Yes, ear drops can cause temporary dizziness through two mechanisms. First, if the drops are cold when applied, the temperature difference can stimulate the vestibular system and cause brief vertigo—this is why warming the bottle before use is recommended. Second, if drops reach the middle ear through a perforation and contact the round window membrane, they can affect inner ear fluid and cause more significant balance disturbances. According to research on cerumen impaction, complete blockage itself can cause vertigo, so drops that initially worsen blockage might temporarily increase dizziness. Persistent or severe vertigo after using ear drops warrants immediate medical evaluation.
Most medical guidelines recommend waiting at least 4-6 hours after using ear drops before swimming. For showering, 1-2 hours is generally sufficient if you’re careful to avoid direct water spray into the treated ear. The concern is twofold: first, water can prematurely flush out medication before it’s had time to work, reducing effectiveness. Second, the ear canal skin is temporarily more vulnerable after ear drop application, and introducing pool or shower water increases infection risk. Some people use petroleum jelly on a cotton ball placed gently at the ear entrance (never inserted into the canal) to protect against water exposure during this waiting period.
Storage requirements relate to medication stability, not safety of extended contact. Refrigerated ear drops (typically certain antibiotic formulations) contain ingredients that degrade at room temperature. But cold drops can cause dizziness when applied, so they should be warmed to body temperature before use by holding the bottle for several minutes. Room-temperature stable drops maintain effectiveness without refrigeration but offer no advantage regarding how long they can safely remain in the ear. Regardless of storage method, application duration guidelines remain the same—the formulation’s ingredients and your eardrum status determine safe contact time, not storage temperature.
The Bottom Line on Ear Drop Duration
Most ear drop mishaps cause temporary discomfort, not permanent damage. The ear’s natural drainage system handles occasional extended exposure reasonably well.
But “reasonably well” isn’t the same as “completely safe.” The specific risks depend on three critical factors: what’s in the drops, the condition of your eardrum, and how long the exposure lasts.
Ototoxic antibiotics with a perforated eardrum present the highest risk scenario. Earwax softeners with an intact eardrum represent the lowest. Most situations fall somewhere in between.
If you’ve used ear drops correctly for several days without improvement—or if symptoms worsen—the problem isn’t the duration of individual applications. The issue might be misdiagnosis, inappropriate medication selection, or a complication requiring different treatment entirely.
That’s when professional evaluation becomes non-negotiable. Audiometry can detect early hearing changes. Otoscopy can identify perforation, infection severity, or underlying structural problems. Tympanometry can assess middle ear function.
The data is clear on one point: according to National Institutes of Health research, cerumen impaction is defined as symptomatic accumulation that prevents diagnostic assessment. If ear drops aren’t resolving the problem, continuing the same approach just increases complication risk.
Look, ears are remarkably resilient structures. They’ve evolved sophisticated self-cleaning mechanisms. But they’re also vulnerable when those mechanisms fail or when we introduce substances that disrupt normal function.
Use ear drops as directed, pay attention to your body’s warning signals, and don’t hesitate to seek professional guidance when something feels off. That’s the approach that protects both immediate comfort and long-term hearing health.