
Quick Summary: When you stop using minoxidil, hair loss typically resumes within 3-6 months, and new growth gained from treatment will gradually shed. Studies show that discontinuing minoxidil results in loss of most non-vellus target scalp hairs within this timeframe. The underlying hair loss condition continues to progress as if treatment never occurred, though no permanent damage results from stopping the medication.
Minoxidil remains one of the most popular over-the-counter treatments for hair loss, with the global market for minoxidil forecasted to exceed $1.2 billion USD by 2024. But what actually happens when someone decides to stop using it?
The question comes up constantly in dermatology clinics and online forums. And for good reason.
Understanding the consequences of discontinuation matters whether someone’s dealing with side effects, tired of the daily routine, or just wondering if they can take a break. Here’s what the research actually shows.
How Minoxidil Works on Hair Follicles
Minoxidil was originally developed as an oral medication for severe hypertension in the 1970s. Physicians noticed an interesting side effect: hair regrowth and generalized hypertrichosis in patients taking the drug.
This observation led to the development of topical formulations specifically for promoting hair growth.
The medication works as a vasodilator, widening blood vessels and potentially improving blood flow to hair follicles. Research suggests minoxidil may also prolong the anagen (growth) phase of the hair cycle and stimulate follicles to transition from telogen (resting) to anagen phase.
But here’s the critical part: minoxidil doesn’t cure the underlying cause of hair loss. It manages symptoms while applied consistently.
The FDA approved 2% minoxidil solutions for over-the-counter use initially, and 5% formulations have since become available when stronger concentrations are needed. Some manufacturers now produce concentrations up to 8% for topical use.
The Timeline: What Happens After Stopping Minoxidil
Research provides clear answers about the discontinuation timeline.
A study evaluating men with male pattern baldness who had been treated with 2% or 3% minoxidil for at least 4 months found specific results. Objective assessments by hair counts showed a mean doubling of non-vellus target scalp hairs while on topical minoxidil.
After stopping? Loss of most of that new growth occurred.
The 3-6 Month Window
Most hair loss reversal happens within 3 to 6 months of discontinuation. The new hairs that grew during treatment gradually return to their previous state.
This timeline aligns with the natural hair growth cycle. Hair doesn’t fall out immediately because follicles cycle through growth phases that last weeks to months.
During the first month after stopping, changes might not be noticeable. By months 2-3, shedding typically becomes apparent. By 6 months, the scalp generally returns to what it would have looked like had treatment never started.
No Additional Damage
One common concern: does stopping minoxidil cause worse hair loss than before starting?
No evidence supports this fear. The hair loss pattern simply resumes its natural progression. The underlying condition—whether androgenetic alopecia or another form of hair loss—continues as it would have without intervention.

Why People Stop Using Minoxidil
A retrospective study assessing compliance to topical minoxidil among patients with androgenetic alopecia revealed striking findings.
The observed discontinuation rate reached 86.3%. That’s a remarkably high percentage.
So what drives people to quit?
Side Effects and Adverse Reactions
Side effects rank among the top reasons for stopping treatment. Common issues include:
- Scalp irritation and itching
- Unwanted facial hair growth (hypertrichosis)
- Dry, flaky scalp
- Contact dermatitis
- Redness at the application site
Research on low-dose oral minoxidil shows hypertrichosis occurs in approximately 15% of patients, with higher incidence in women and patients with higher doses.
The FDA has also become aware of reports of adverse events involving compounded topical finasteride products—sometimes combined with minoxidil—that potentially put consumers at risk.
Lack of Visible Results
Treatment efficacy varies considerably between individuals.
Available data from studies shows disappointing response rates for many users. In clinical trials: 60% of men in one study did not experience hair growth, 38% of men in another study did not report hair growth, and 81% of women in a third study did not report significant hair growth.
When results don’t materialize after months of consistent application, motivation to continue naturally wanes.
Time and Inconvenience
Daily application requires commitment. Twice-daily applications for foam or liquid formulations mean integrating the routine into morning and evening schedules indefinitely.
The medication needs at least 12 months to properly assess treatment efficacy, according to research emphasizing patient education. Many people discontinue before reaching this milestone.
Hair styling becomes more complicated. The product needs time to dry. It can leave residue or make hair look greasy.
Cost Considerations
Long-term use creates ongoing expenses. Over-the-counter formulations require continuous repurchasing. For individuals without insurance coverage for hair loss treatments, the cumulative cost becomes a factor in discontinuation decisions.
Initial Shedding Phase
Research confirms that hair shedding increases temporarily after starting topical minoxidil use. This counterintuitive initial effect—losing more hair when trying to prevent hair loss—causes some people to stop treatment prematurely.
The shedding actually indicates the medication is working, pushing follicles into active growth phases. But without understanding this mechanism, the experience can be alarming enough to trigger discontinuation.
| Discontinuation Reason | Impact Level | Typical Timeline |
|---|---|---|
| Side effects (irritation, unwanted hair growth) | High | 1-3 months |
| Lack of visible results | High | 6-12 months |
| Daily application inconvenience | Medium | 3-6 months |
| Cost concerns | Medium | Variable |
| Initial shedding phase | Medium | 1-2 months |
The Shedding Phase After Discontinuation
Understanding what happens during the post-treatment shedding phase helps set realistic expectations.
Hair doesn’t fall out all at once. The process mirrors the gradual way it grew during treatment—just in reverse.
Telogen Effluvium Response
Stopping minoxidil can trigger a telogen effluvium-like response. This means an increased proportion of hair follicles shift into the telogen (resting/shedding) phase simultaneously.
The hairs that minoxidil kept in active growth phase transition to rest and eventually shed. This concentrated shedding period can be more noticeable than the gradual thinning that occurred before starting treatment.
But this isn’t “extra” hair loss. It’s simply the loss of treatment-dependent growth occurring in a compressed timeframe.
Variability in Individual Response
Not everyone experiences the same degree of shedding after stopping. Factors include:
- Duration of treatment
- How well the medication worked initially
- Underlying cause and severity of hair loss
- Individual follicle sensitivity
- Whether other treatments are being used concurrently
Someone who had minimal response to minoxidil will likely notice less dramatic changes after stopping compared to someone who achieved significant regrowth.
Can Treatment Be Restarted Later?
This question matters for people considering a break from treatment or those who stopped but want to resume.
The short answer? Minoxidil can be restarted, but response may vary.
Effectiveness After Restarting
Some research suggests that restarting minoxidil after a gap may still produce results, though potentially not identical to the initial response. Hair follicles don’t develop permanent resistance to the medication.
However, the underlying hair loss condition continues progressing during the break. More follicles may have miniaturized or become inactive during the treatment gap, which could affect overall regrowth potential.
Starting From Scratch
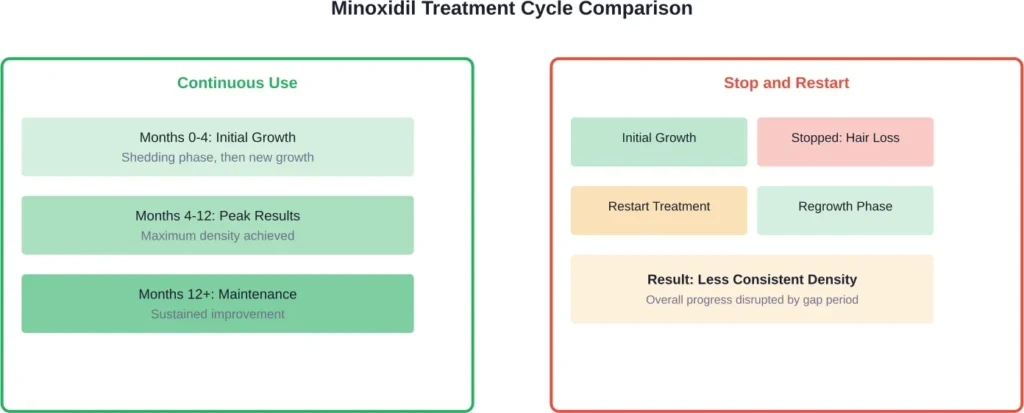
Restarting treatment essentially means beginning the process again. The initial shedding phase might recur. The waiting period to see results—typically 3-4 months minimum—restarts.
Consistency matters more than intermittent use. Hair follicles need continuous stimulation to maintain treatment-dependent growth.
Alternatives to Minoxidil
Several other treatment options exist for managing hair loss, each with different mechanisms and considerations.
Finasteride (Oral)
Two FDA-approved oral finasteride products exist for different indications: Proscar (approved June 19, 1992) and Propecia (approved December 19, 1997). For male pattern hair loss, finasteride works by inhibiting the enzyme that converts testosterone to dihydrotestosterone (DHT), a hormone that shrinks hair follicles.
Unlike minoxidil’s topical vasodilating action, finasteride addresses hormonal factors in androgenetic alopecia. Some providers prescribe it for pattern hair loss in men, though it carries its own side effect profile including potential sexual dysfunction.
Oral Spironolactone
This prescription medication option for women can prevent further hair loss and increase hair thickness. Studies show that oral spironolactone is effective in about 40% of women who have female pattern hair loss.
Spironolactone functions as an androgen blocker, reducing the effects of male hormones that can contribute to hair thinning in women.
Low-Dose Oral Minoxidil
Recent studies demonstrate that low-dose oral minoxidil can be a safe and effective treatment for numerous hair disorders including male-patterned and female-patterned hair loss.
Practical advantages include eliminating the daily topical application routine. However, systemic absorption means different side effect considerations compared to topical use.
Corticosteroid Injections
This is considered the most effective treatment for people who have a few patches of hair loss. In one study of 127 patients with patchy hair loss, more than 80% who were treated with corticosteroid injections had at least half of their hair regrow within 12 weeks.
This approach targets the autoimmune component of alopecia areata rather than androgenetic alopecia.
Platelet-Rich Plasma (PRP) and Other Emerging Options
Various treatment modalities continue to be researched and used in clinical practice, including platelet-rich plasma injections, laser therapy, and microneedling combined with topical treatments.
Evidence quality varies across these interventions. A few studies have shown that microneedling combined with 5% minoxidil twice daily produces better results than minoxidil alone after 12 weeks of treatment in men with mild or moderate hereditary hair loss.
| Treatment Option | Administration | Primary Mechanism | Best For |
|---|---|---|---|
| Topical Minoxidil | Applied to scalp 1-2x daily | Vasodilation, growth phase extension | Pattern hair loss (male/female) |
| Oral Finasteride | Daily pill | DHT reduction | Male pattern hair loss |
| Oral Spironolactone | Daily pill | Androgen blocking | Female pattern hair loss |
| Corticosteroid Injections | Clinical injections | Immune modulation | Alopecia areata |
| Low-dose Oral Minoxidil | Daily pill | Systemic vasodilation | Multiple alopecia types |
Medical Guidance on Discontinuation
Board-certified dermatologists emphasize the importance of educating patients regarding treatment side effects and the need to use minoxidil for a minimum of 12 months to assess treatment efficacy.
Professional guidance before stopping treatment can help individuals:
- Understand realistic expectations for what happens after discontinuation
- Explore alternative treatments if side effects are the primary concern
- Adjust application methods or formulations to improve tolerability
- Develop a transition plan if switching to different medications
Dermatologists have in-depth knowledge about the many causes of hair loss and experience treating diverse causes. A proper diagnosis ensures treatment targets the actual underlying condition.
When Stopping Makes Sense
Discontinuation is sometimes the appropriate choice:
- Severe or persistent side effects that affect quality of life
- Allergic reactions or contact dermatitis
- Pregnancy or planning pregnancy (minoxidil safety during pregnancy is not established)
- No response after 12+ months of consistent use
- Medical conditions that contraindicate continued use
The decision should be informed rather than impulsive.
Managing Expectations and Long-Term Planning
Realistic expectations form the foundation of any hair loss treatment approach.
Minoxidil doesn’t work for everyone. Even when it does work, regrowth is typically partial rather than complete restoration. The medication requires indefinite use to maintain results.
Compliance Challenges
The high discontinuation rate—86.3% in research studies—reflects real-world challenges with topical minoxidil compliance. Clinical use is limited by substantially low compliance even in absence of adverse effects.
Understanding these statistics helps normalize the struggle many people face with consistent application.
Combination Approaches
Many dermatologists recommend combination approaches for pattern hair loss. Using multiple treatments with different mechanisms may produce better results than monotherapy.
For example, combining minoxidil with finasteride addresses both the vasodilating/growth-promoting angle and the hormonal component of androgenetic alopecia.
However, the FDA has become aware of some compounders and telemedicine platforms marketing topical formulations of finasteride either alone or combined with minoxidil. Currently, there is no FDA-approved topical formulation of finasteride. There were 32 cases of adverse events reported to the FDA Adverse Event Reporting System between 2019 and 2024 related to compounded topical finasteride products.
Psychological and Emotional Considerations
Hair loss affects more than physical appearance. The emotional impact matters.
Stopping treatment—and experiencing renewed shedding—can be psychologically difficult. Some people report anxiety or depression related to visible hair thinning.
Support resources include:
- Hair loss support groups and online communities
- Counseling for body image concerns
- Dermatology clinics with comprehensive hair disorder programs
- Educational resources from organizations like the American Academy of Dermatology
Addressing the emotional component alongside the physical treatment creates a more holistic approach.
Special Populations and Discontinuation
Certain groups face unique considerations when stopping minoxidil.
Women of Childbearing Age
Minoxidil safety during pregnancy hasn’t been established through adequate controlled studies. Women who become pregnant or plan pregnancy typically need to discontinue treatment.
Discussing transition plans with healthcare providers before stopping helps manage the hair loss that will likely follow.
Individuals With Cardiovascular Concerns
Though rare with topical use, systemic absorption can occur. One historical concern involves rebound hypertension following minoxidil withdrawal in patients using high-dose oral formulations for severe hypertension.
For individuals using low-dose oral minoxidil for hair loss, cardiovascular monitoring may be recommended during treatment and potentially during discontinuation.
Patients With Multiple Medications
Those using minoxidil alongside other hair loss treatments need coordinated discontinuation planning. Stopping all treatments simultaneously versus tapering one at a time produces different outcomes.
Frequently Asked Questions
Research shows that discontinuing minoxidil results in loss of most non-vellus target scalp hairs that grew during treatment. The hair gained from minoxidil is treatment-dependent, so it gradually sheds over 3-6 months after stopping. Hair typically returns to what it would have looked like had treatment never been used.
Minoxidil can be restarted after a break, though response may vary from the initial treatment period. The underlying hair loss condition continues progressing during any gap in treatment, potentially affecting regrowth results. Restarting essentially means beginning the treatment cycle again, including the initial waiting period for visible results.
The shedding phase after discontinuation typically occurs over a 3-6 month window. Hair doesn’t fall out all at once but gradually transitions through normal growth cycles. Most people notice the return to baseline hair density by 6 months after stopping treatment.
No evidence suggests that stopping minoxidil causes additional damage or worsens hair loss beyond the natural progression of the underlying condition. The hair loss pattern simply resumes as it would have without treatment. Any perception of worse loss is typically due to the concentrated shedding period rather than actual increased hair loss.
A study on compliance found an 86.3% discontinuation rate among patients with androgenetic alopecia. Common reasons include side effects like scalp irritation and unwanted facial hair growth, lack of visible results after months of use, daily application inconvenience, cost considerations, and concern about the initial shedding phase that occurs when starting treatment.
Several alternatives exist depending on the type of hair loss. Options include oral finasteride for male pattern baldness, oral spironolactone for female pattern hair loss (effective in about 40% of women), corticosteroid injections for alopecia areata, and low-dose oral minoxidil. Combination approaches using multiple treatments with different mechanisms may also be considered. Consultation with a board-certified dermatologist helps identify appropriate alternatives.
Consulting a dermatologist before discontinuing provides valuable guidance about what to expect, potential alternative treatments, and whether the reasons for stopping might be addressed through formulation changes or application adjustments. Medical guidance is particularly important for individuals with cardiovascular conditions, those who are pregnant or planning pregnancy, and people using multiple hair loss treatments simultaneously.
Conclusion
Stopping minoxidil triggers a predictable sequence of events backed by clinical research. Hair gained during treatment gradually sheds over 3-6 months as follicles return to their pre-treatment state.
The underlying hair loss condition resumes its natural progression. No permanent damage occurs from discontinuation, though the loss of treatment-dependent growth can be emotionally difficult.
High discontinuation rates—reaching 86.3% in research studies—reflect real challenges with compliance, side effects, limited efficacy in some individuals, and the ongoing commitment required.
For those considering stopping minoxidil, understanding the timeline and alternatives helps create informed decisions. Whether stopping due to side effects, lack of results, or personal choice, knowing what to expect removes some uncertainty from the process.
Consultation with a board-certified dermatologist provides personalized guidance for managing hair loss through treatment transitions. Effective approaches to hair loss begin with accurate diagnosis and realistic expectations about any treatment’s capabilities and limitations.
Visit a dermatology professional to discuss your specific hair loss pattern and explore all available treatment options that match your needs and lifestyle.