
Quick Summary: Taking PEP (post-exposure prophylaxis) without actual HIV exposure is generally unnecessary and potentially wasteful of medical resources, though not harmful if monitored properly. PEP is designed as emergency medication for those who may have been exposed to HIV within the past 72 hours, not for preventive use without exposure. If there’s uncertainty about exposure risk, consulting a healthcare provider is essential—they’ll assess the situation and determine if PEP is warranted.
The anxiety following a potential HIV exposure can be overwhelming. Sometimes, that fear leads people to seek PEP even when their actual risk was minimal or nonexistent. But what really happens if someone takes this emergency medication without genuine exposure?
Understanding the answer requires looking at what PEP is, how it works, and the medical implications of using powerful antiretroviral drugs when they’re not medically necessary.
Understanding PEP: What It Is and How It Works
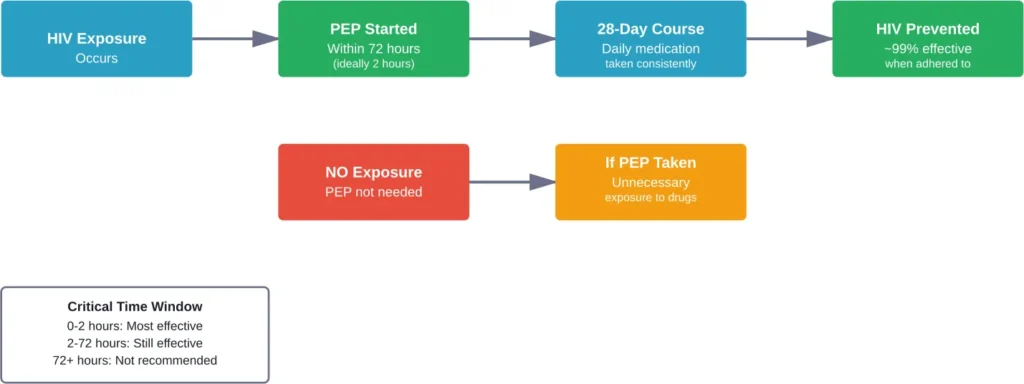
According to the CDC, PEP (post-exposure prophylaxis) is the use of antiretroviral medication to prevent HIV in a person without HIV who may have been exposed to the virus. It’s designed as emergency intervention, not routine prevention.
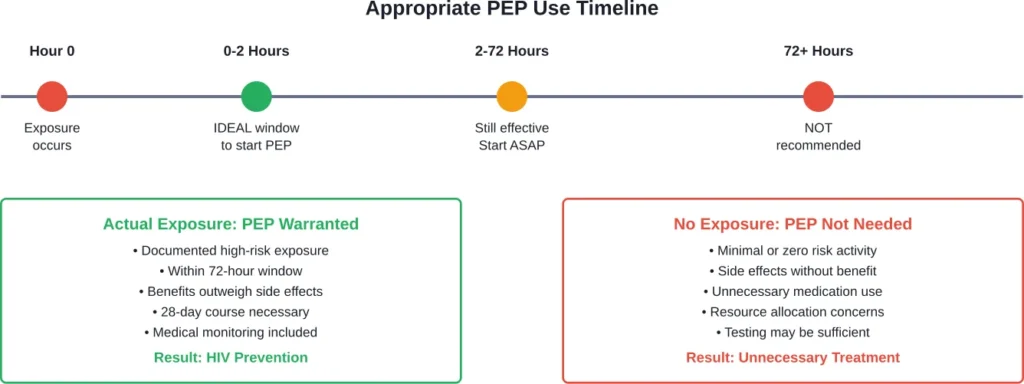
PEP works by preventing HIV from entering cells in the body and stopping the virus from establishing a persistent infection. The medication needs to be started quickly—ideally within 2 hours of exposure but no later than 72 hours after potential exposure—because effectiveness decreases significantly with time.
The typical PEP regimen involves taking antiretroviral drugs for 28 consecutive days. Most commonly prescribed combinations include medications like tenofovir, emtricitabine, and raltegravir or dolutegravir.
The Science Behind PEP Effectiveness
Research shows PEP can be highly effective when used appropriately. Clinical studies and observational data demonstrate that rapid administration of antiretroviral medications after exposure can prevent HIV infection from taking hold.
Modeling data on HIV PEP pharmacokinetics suggests that without any drugs, HIV infection becomes irreversible two to five days after exposure. With a combination of antiretroviral medications, PEP creates a protective barrier during this critical window.
But here’s the thing—PEP isn’t 100% effective even with genuine exposure. There have been very few reports of HIV infection after proper use of PEP, but the medication works best when there’s actual virus to prevent from replicating.
What Actually Happens When You Take PEP Without Exposure
So what occurs if someone takes PEP when they haven’t actually been exposed to HIV? The physical effects come down to several key factors.
Medication Side Effects Without Therapeutic Benefit
Antiretroviral drugs used in PEP regimens are powerful medications designed to suppress viral replication. When taken without actual virus present, the body still experiences the medication’s effects—just without the protective benefit.
Common side effects of PEP medications include nausea, fatigue, headache, and diarrhea. Some people experience more significant reactions like dizziness, difficulty sleeping, or mood changes. These side effects occur whether or not HIV is present in the system.
The difference? When PEP is medically necessary, these side effects are justified by the critical need to prevent HIV infection. Without genuine exposure, someone experiences potential discomfort and side effects without any corresponding benefit.
Medical Monitoring and Healthcare Resource Use
Proper PEP treatment requires baseline assessment and ongoing monitoring. According to CDC guidelines, people beginning PEP need baseline HIV testing, kidney function tests, and potentially other laboratory work depending on their health status.
This medical oversight continues throughout the 28-day course. Healthcare providers monitor for side effects, check medication adherence, and conduct follow-up HIV testing at specific intervals after completing the regimen.
When PEP is taken without actual exposure, all these medical resources are utilized without addressing a real health threat. In healthcare systems with limited resources, this can potentially reduce availability for those with genuine need.
The Risk Assessment Question
Here’s where it gets complicated. HIV risk assessment isn’t always straightforward. What seems like “no exposure” to one person might represent genuine risk to a healthcare provider with more complete information.
Real talk: the risk of catching HIV from a single exposure varies enormously based on the type of exposure, viral load of the source (if known), and other factors. According to available data, transmission risk from one exposure can be less than 1 in 100, and often even lower—sometimes less than 1 in 1,000 or 1 in 10,000.
But doctors assess risk based on clinical guidelines, not assumptions. They consider factors like whether the exposure involved mucous membranes, broken skin, or percutaneous injury, and whether the source individual has HIV or unknown status.
| Exposure Type | Estimated Transmission Risk | PEP Recommendation |
|---|---|---|
| Receptive anal intercourse with HIV+ partner | Higher risk (varies by viral load) | Strongly recommended |
| Insertive vaginal intercourse with unknown status | Low to moderate risk | Consider based on prevalence |
| Condom-protected sex, no breakage | Minimal to zero risk | Generally not recommended |
| Oral sex without ejaculation | Very low risk | Rarely recommended |
| Needle stick with HIV+ blood (healthcare) | Approximately 0.3% | Recommended |
| Kissing, touching, no fluid exchange | Zero risk | Not recommended |
When Uncertainty Leads to PEP Use
The psychological component of potential HIV exposure can’t be dismissed. Anxiety after a sexual encounter or other exposure can be intense, even when objective risk is low.
Many sexual health clinics and emergency departments report seeing patients requesting PEP when their exposure doesn’t meet clinical criteria for recommendation. Doctors face a challenging balance—addressing patient anxiety while ensuring appropriate medication use.
Some healthcare providers may prescribe PEP even for lower-risk exposures if the patient is highly anxious and committed to taking the full 28-day course. The reasoning: while not strictly medically necessary, completing PEP is unlikely to cause serious harm, and the psychological benefit of taking action may be significant.
That said, this isn’t universal practice. Clinical guidelines from the CDC specify that PEP is not recommended for people whose exposure occurred more than 72 hours before seeking treatment, as it’s unlikely to be effective after this window.
The Difference Between PEP and PrEP
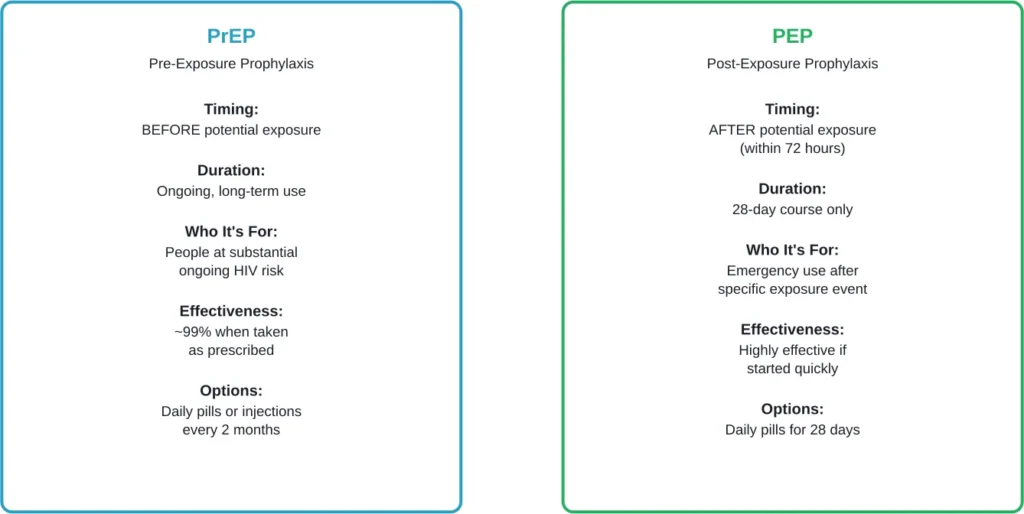
Confusion sometimes arises between PEP (post-exposure prophylaxis) and PrEP (pre-exposure prophylaxis). They’re different interventions with different purposes.
According to the CDC, PrEP is medication taken by people without HIV to prevent infection before potential exposure occurs. When taken as prescribed, both oral and injectable PrEP reduce the risk of getting HIV from sex by about 99%. (Note: This pertains to PrEP, not PEP)
PrEP is designed for ongoing use by people at substantial risk—like those with HIV-positive partners not on treatment, people with multiple partners in high-prevalence areas, or those who inject drugs. It’s preventive medicine taken regularly, not emergency treatment.
PEP, by contrast, is emergency intervention after a specific exposure event. Taking PEP without exposure is fundamentally different from taking PrEP as ongoing prevention for someone at substantial risk.
Medical and Ethical Considerations
The question of taking PEP without exposure raises broader issues about medical resource allocation and appropriate medication use.
Antiretroviral Resistance Concerns
One concern with unnecessary antiretroviral use is potential contribution to drug resistance. While this is more of a population-level concern than an individual risk, it’s worth understanding.
HIV develops resistance when exposed to antiretroviral drugs but not fully suppressed. This typically happens when someone with HIV takes medications inconsistently or at suboptimal doses.
For someone without HIV taking PEP, resistance isn’t an issue because there’s no virus present to develop resistance. However, if someone unknowingly had HIV at the start of PEP (due to testing during the window period), taking a partial regimen could theoretically contribute to resistance.
This is why proper baseline testing is so critical before starting PEP.
Access and Cost Issues
PEP medications can be expensive without insurance coverage. The 28-day regimen may cost hundreds or even thousands of dollars at retail prices, though many insurance plans and state Medicaid programs cover PEP, according to CDC information.
Programs exist to help cover PEP costs for those without insurance, but resources aren’t unlimited. When someone uses PEP without genuine medical need, it potentially diverts resources from others with actual exposure risk.
That said, individual cases are complex. Healthcare providers must balance resource considerations against patient needs and clinical judgment.
Psychological Impact and Anxiety Management
The fear following a potential HIV exposure can be psychologically devastating. Understanding this anxiety is important for comprehensive care.
Many people seeking PEP are experiencing acute stress related to the exposure event. This might involve sexual assault, a condom breaking with a partner of unknown status, or occupational exposure for healthcare workers.
In these situations, PEP serves both a medical and psychological function. Even when objective risk is low, the act of taking medication provides a sense of agency and control during a frightening time.
However, repeatedly seeking PEP for low-risk or no-risk exposures might indicate underlying anxiety that would be better addressed through mental health support rather than continued medication use.
When Anxiety Outweighs Risk
Healthcare providers sometimes encounter patients requesting PEP for exposures that carry essentially zero HIV risk—like protected sex with no condom breakage, or contact that didn’t involve any exchange of bodily fluids.
In these cases, education about HIV transmission becomes crucial. Understanding which activities do and don’t pose risk can help reduce unnecessary anxiety and medication use.
But this education needs to be delivered with compassion, not dismissiveness. The fear is real, even when the risk isn’t.
Alternative Approaches for Low-Risk Situations
For people experiencing anxiety after low-risk exposures, several alternatives to PEP exist.
Baseline and Follow-Up Testing
One approach involves baseline HIV testing followed by appropriate follow-up testing based on the window period of modern tests. Fourth-generation HIV tests can detect infection as early as 18-45 days after exposure, though testing at 90 days provides definitive results.
This testing approach provides reassurance without exposing someone to 28 days of medication side effects when PEP isn’t medically indicated.
Transitioning to PrEP for Ongoing Risk
Sometimes a person seeking PEP actually needs PrEP. If someone has repeated potential exposures or ongoing risk factors, pre-exposure prophylaxis might be more appropriate than emergency post-exposure treatment.
According to recent CDC guidance, healthcare providers should offer PrEP medication and methods of administration to meet patients’ needs. This includes newer options like injectable cabotegravir given every two months, or lenacapavir administered twice yearly.
The shift from reactive PEP use to proactive PrEP can provide better protection and reduce the cycle of exposure anxiety.
| Situation | PEP Appropriate? | Alternative Recommendation |
|---|---|---|
| Condom broke with HIV+ partner not virally suppressed | Yes | Start immediately, consider PrEP long-term |
| Unprotected sex, partner status unknown, high-prevalence area | Likely yes | Risk assessment by provider |
| Protected sex, no condom failure | No | Reassurance, testing if needed for peace of mind |
| Repeated exposures over time | No (for repeated pattern) | Transition to PrEP for ongoing protection |
| Occupational needle stick, source HIV+ | Yes | Immediate occupational health consultation |
| Kissing or touching only, no fluid exchange | No | Education about zero-risk activities |
The Clinical Decision-Making Process
Healthcare providers use specific criteria to determine when PEP is warranted. Understanding this process helps clarify when medication is truly needed.
According to clinical guidelines, PEP prescription involves assessing several factors. Was the exposure within the 72-hour window? What type of exposure occurred? What’s known about the source individual’s HIV status?
Providers also consider local HIV prevalence, the specific nature of the exposure, and patient factors that might affect medication tolerance or absorption.
This comprehensive assessment sometimes reveals that what a patient perceived as significant exposure actually carries minimal risk. Conversely, it might identify higher risk than the patient realized.
Baseline Testing Before PEP
One critical component is baseline HIV testing. PEP should not be started in someone who already has HIV—they need full antiretroviral therapy, not a 28-day prophylactic regimen.
But here’s the challenge: if someone was infected shortly before seeking PEP, standard HIV tests might not detect the infection yet due to the window period. This is why follow-up testing after completing PEP is essential.
If someone takes PEP without actual exposure, they’ll test negative at baseline and remain negative throughout—because they never had HIV to begin with. The PEP didn’t prevent anything; there was nothing to prevent.
What Healthcare Providers Recommend
Medical professionals consistently emphasize that PEP decisions should involve clinical consultation, not self-assessment alone.
If there’s uncertainty about whether an exposure occurred or whether it poses HIV risk, the recommendation is clear: seek medical evaluation quickly. Emergency departments, sexual health clinics, and urgent care centers can provide assessment.
Many areas now have specialized sexual health services offering same-day PEP evaluation and prescription when appropriate. Some locations provide PEP starter packs to begin treatment immediately while full assessment continues.
The key message from healthcare providers: don’t delay seeking evaluation due to uncertainty. Let medical professionals assess risk and determine whether PEP is warranted. The 72-hour window means every hour counts when genuine exposure has occurred.
Long-Term Health Implications
For most people, taking a single 28-day course of PEP causes no long-term health effects. The medications clear from the system after stopping, and any side effects typically resolve.
However, some medications used in PEP regimens can affect kidney function or bone density with prolonged use. For a single 28-day course, these effects are minimal. But repeated unnecessary use of PEP could theoretically pose cumulative risks.
This is another reason why people with ongoing HIV risk are better served by structured PrEP programs with appropriate medical monitoring rather than repeated PEP courses.
Medication Interactions and Health Conditions
PEP medications can interact with other drugs and may not be suitable for everyone. People with certain kidney or liver conditions might need modified regimens or closer monitoring.
Taking PEP without medical supervision—or without disclosure of other medications or health conditions—could pose risks. This is why PEP should always involve healthcare provider consultation and monitoring.
Frequently Asked Questions
PEP medications can cause side effects like nausea, fatigue, and headaches regardless of whether HIV exposure occurred. For most people, a 28-day course won’t cause lasting harm, though some medications may affect kidney function or bone density. The primary concern is experiencing medication side effects without any corresponding benefit. Anyone taking PEP should be under medical supervision to monitor for adverse effects.
Healthcare providers assess several factors including the type of exposure, timing (must be within 72 hours), source individual’s HIV status or risk factors, local HIV prevalence, and the patient’s health status. They evaluate whether the exposure involved blood, semen, vaginal fluids, or other infectious materials, and whether it contacted mucous membranes or broken skin. This comprehensive risk assessment determines whether PEP’s benefits outweigh the risks of medication side effects.
PEP is emergency medication taken for 28 days after a specific exposure event within 72 hours. Taking it without exposure means experiencing side effects without preventing anything. PrEP, by contrast, is designed for ongoing prevention in people at substantial ongoing risk—it’s taken continuously before exposures occur. Someone with repeated potential exposures should discuss PrEP with their healthcare provider rather than using PEP repeatedly. According to the CDC, PrEP reduces HIV risk by about 99% when taken as prescribed.
Insurance coverage depends on medical necessity determination. If a healthcare provider assesses the situation and prescribes PEP based on clinical judgment, insurance may cover it. However, if documentation clearly shows no risk exposure occurred, coverage might be denied. Most insurance plans and state Medicaid programs cover PEP when medically appropriate. Some areas offer programs to help cover costs for uninsured individuals with documented exposure risk.
If someone truly has no HIV infection, they cannot develop resistance because there’s no virus present to become resistant. The concern arises if someone unknowingly had HIV when starting PEP—perhaps infected just before the exposure event they’re worried about, during the testing window period. In that case, taking incomplete HIV treatment could theoretically contribute to resistance. This is why baseline HIV testing before PEP and follow-up testing afterward are critical components of proper PEP protocols.
Yes—uncertainty about exposure risk warrants professional medical evaluation, especially within the 72-hour window. Don’t try to assess risk yourself. Contact an emergency department, sexual health clinic, or urgent care facility immediately. Healthcare providers can conduct proper risk assessment and determine whether PEP is warranted. The evaluation itself provides valuable information and peace of mind, and if PEP is needed, starting quickly maximizes effectiveness. Every hour counts when genuine exposure has occurred.
If definitive information becomes available that the source individual is HIV-negative (confirmed through testing, not just assumption), PEP can be discontinued as it’s no longer necessary. Consult with the prescribing healthcare provider before stopping—they may recommend completing a shorter course or confirm that stopping is appropriate. This situation demonstrates why source testing, when possible, is valuable in PEP decision-making. However, waiting for source test results shouldn’t delay starting PEP if the exposure warrants it.
The Bottom Line on PEP Without Exposure
Taking PEP without genuine HIV exposure subjects someone to medication side effects without providing any protective benefit. It’s not physically harmful in most cases, but it represents unnecessary medication use and potentially diverts resources from those with actual need.
The critical message: PEP decisions should involve healthcare professionals, not self-assessment. Medical providers can accurately assess exposure risk using clinical guidelines and determine whether emergency prophylaxis is warranted.
For people experiencing repeated anxiety about potential exposures, addressing the underlying concerns—whether through education about transmission risk, mental health support, or transitioning to PrEP for ongoing prevention—provides better long-term outcomes than repeated unnecessary PEP courses.
HIV prevention has never been more effective, with multiple tools available. PEP serves a vital role in that prevention toolkit, but like any medical intervention, it works best when used appropriately for its intended purpose.
If you’re uncertain about whether a potential exposure warrants PEP, seek medical evaluation immediately. The 72-hour window means time is critical, and professional assessment provides both appropriate medical care and peace of mind.