
Quick Summary: Letting a baby cry is sometimes acceptable when done responsibly. Research shows that brief, monitored crying during sleep training doesn’t harm attachment or development when basic needs are met. However, prolonged, unattended crying can be stressful for both baby and parents. The key is responding to genuine distress while allowing brief periods for self-soothing in safe situations.
Few parenting questions generate more anxiety than this one. The moment your baby starts crying and you’re standing there, exhausted and uncertain—should you rush in immediately or wait a few minutes?
The internet hasn’t made this easier. One expert swears by immediate response. Another insists babies need to learn self-soothing. Parents report success with both approaches, while others describe either method as damaging.
So what does the actual research say? And more importantly, what should you do tonight when your baby won’t settle?
Understanding Why Babies Cry
Before addressing whether it’s acceptable to let crying continue, it helps to understand what’s happening. Crying is the only communication tool newborns possess. It’s typical for newborns to cry 1 to 4 hours daily—that’s completely normal development, not a sign that something’s wrong with your baby or your parenting.
Babies cry for concrete reasons: hunger, discomfort, tiredness, overstimulation, or the need for closeness. Newborns sleep about 16 to 17 hours daily in fragmented periods—waking frequently during sleep cycles is biologically normal, not a problem to fix. A baby might cry simply because they’re exhausted but haven’t learned to transition into sleep independently.
Here’s where things get complicated. Up to 40% of parents report infant sleep disturbance as concerning. Between 20% and 30% of infants experience night awakenings during their first two years. Meanwhile, 50% to 75% of infants sleep through the night at 12 weeks, and 90% manage this by 6 months.
That leaves a substantial number of families dealing with persistent sleep challenges well beyond the newborn period.
What “Crying It Out” Actually Means
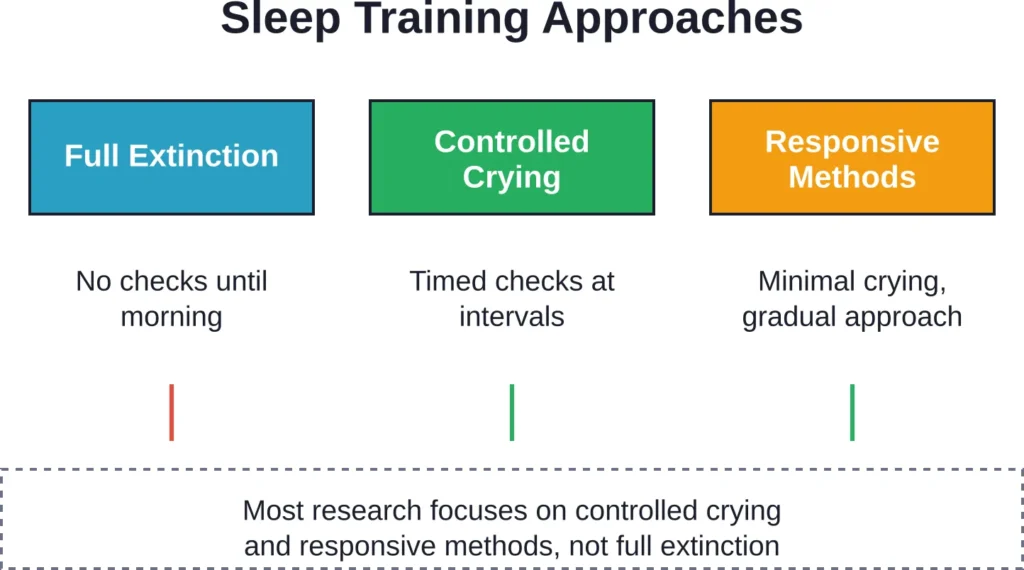
The phrase gets thrown around loosely, often conflating several distinct approaches. Sleep training, or controlled crying, typically involves parents responding to their infant’s cry at increasing time intervals to allow independent settling.
This isn’t the same as abandoning a screaming baby for hours. Most methods involve checking on the baby at regular intervals—perhaps every 5, then 10, then 15 minutes. Parents offer reassurance without picking up the baby, then leave again.
According to HealthyChildren.org (American Academy of Pediatrics), parents should not rush in to soothe a crying baby and babies need time to put themselves back to sleep.
But wait. There’s also full extinction (rarely recommended), where parents don’t return until morning. Then there are gentler methods that involve minimal crying. And countless variations in between.
No wonder parents are confused.
What the Research Actually Shows
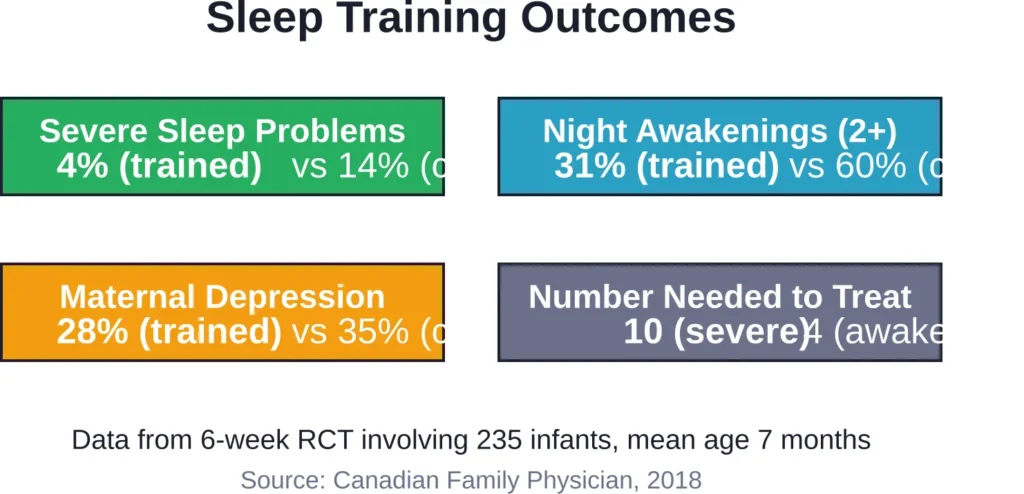
The evidence base is more nuanced than social media would suggest. A study published in the Canadian Family Physician journal examined 235 infants with a mean age of 7 months who had sleep problems defined as 2 or more awakenings per night on 5 or more nights weekly.
After 6 weeks of sleep training, only 4% of infants in the intervention group had severe sleep problems compared to 14% in the safety education control group. The number needed to treat for severe sleep problem reduction was 10—meaning for every 10 families who tried sleep training, approximately one child with severe sleep problems improved compared to control.
Diary-recorded awakenings showed 31% of sleep-trained infants still had 2 or more awakenings compared to 60% in the control group. The number needed to treat for reducing awakenings was 4.
Another cluster randomized controlled trial involving 328 families with infants averaging 7 months found that 56% of mothers in the intervention group reported infant sleep problems at 10 months, compared to 68% receiving usual care. Maternal mood scales improved in intervention groups, with some studies showing lower depression scores in mothers receiving successful sleep interventions.
The maternal mood improvements are significant. Research consistently shows that mothers with the lowest baseline depression scores benefit the most from successful sleep interventions.
The Attachment Question
This is where anxiety peaks. Will letting your baby cry damage your bond or harm their psychological development?
Research examining controlled crying methods with parental checks found no association with adverse behavioral development or attachment. Infants and toddlers who experienced responsive and sensitive care throughout their development tend to develop into socially competent preschoolers, but brief crying episodes during sleep training don’t appear to override overall patterns of responsive care.
That said—and this matters—these studies examined controlled crying approaches with checks and limits, not prolonged unattended distress. There’s a meaningful difference between 10 minutes of crying with a check and hours of screaming alone.
Stress Levels and Cortisol
Some opponents of crying-based methods cite stress hormone concerns. A pilot study examined stress responses during responsive sleep interventions compared to extinction methods, measuring stress hormones in mothers and infants.
Responsive methods—which involve minimal crying—showed different stress patterns than extinction approaches. However, the research notes that up to 40% of parents report infant sleep disturbance as concerning, creating parental stress that also affects the infant.
The relationship between infant crying and stress is complicated. Brief cortisol elevations during learning new skills (including sleep) differ from chronic stress exposure. Context matters enormously.
When Crying Is Acceptable (and When It Isn’t)
The critical distinction isn’t whether crying happens—it’s the context, duration, and response pattern.
Crying is generally considered acceptable when:
- All basic needs have been checked and met (fed, clean diaper, comfortable temperature, not in pain)
- The baby is in a completely safe sleep environment on their back
- The duration is brief and monitored—typically 10 to 15 minutes maximum for young infants
- The parent checks in at regular intervals
- This is part of a consistent, age-appropriate sleep teaching approach
- The baby is at least 4 to 6 months old (sleep training methods aren’t typically recommended for infants younger than 4 to 6 months)
Crying becomes problematic when:
- The baby is very young (under 4 months) and still establishing feeding and trust
- Basic needs haven’t been addressed
- The crying continues for extended periods without any check or comfort
- The baby is sick or in genuine distress
- The crying is punishment-based rather than teaching-based
- Parents are using crying methods out of anger or frustration rather than as a deliberate strategy
Sleep training methods work best when infants are developmentally ready. Circadian rhythms begin developing around 10 to 12 weeks, but most experts recommend waiting until at least 4 to 6 months before attempting formal sleep training.
Age-Appropriate Expectations
Understanding normal sleep development prevents unnecessary intervention. Total sleep needs decrease as babies grow, with variation among individual infants.
These are averages; individual variation is normal. Expecting a 2-month-old to sleep through the night sets everyone up for frustration. That baby is doing exactly what their biology demands. Interventions make sense when sleep problems persist beyond developmental norms and genuinely impact family functioning.
| Age | Total Daily Sleep | Night Sleep Development | Sleep Training |
|---|---|---|---|
| Newborn | 16-17 hours | Fragmented, 1-2 hour cycles | Not recommended |
| 16 weeks | 14-15 hours | 50-75% sleep through night | Not typically recommended |
| 6 months | 13-14 hours | 90% sleep through night | Can be appropriate if needed |
| 12+ months | 12-14 hours | Most sleep through consistently | Appropriate if sleep issues persist |
What to Do Instead When You Can’t Handle the Crying
Real talk: sometimes you’re at your breaking point. The baby has been screaming for what feels like hours. You’ve tried everything. You’re exhausted, maybe even feeling angry.
This is when knowing it’s acceptable to put the baby down safely becomes crucial.
According to the American Academy of Pediatrics, if you’ve tried to calm your crying baby but nothing works, take a moment for yourself. Place the baby on their back in a safe sleep space—crib or bassinet with no loose bedding. Leave the room. Take a deep breath and count to 10. Call a friend or family member for support.
Crying won’t harm your baby in the short term. Shaking a baby or handling them roughly out of frustration causes catastrophic injury. Taking a 10-minute break to calm yourself is the safer choice.
When you’re sleep-deprived and mentally exhausted, crying becomes exponentially harder to handle. Set an alarm on your phone to go off every few minutes if you’re worried about falling asleep while feeding. Accept help from partners, family, or friends.
Community discussions consistently emphasize this point: protecting your mental health isn’t selfish—it’s essential for your baby’s wellbeing. A caregiver at their breaking point cannot provide responsive, sensitive care.
Alternatives to Crying-Based Methods
Not every family needs sleep training, and not every family who needs better sleep wants to use crying methods. Responsive alternatives exist.
Gradual approaches might involve sitting next to the crib while the baby falls asleep, then slowly moving your chair farther away over successive nights. Or picking the baby up when they cry, putting them down drowsy but awake, and repeating as needed.
These methods often take longer and require more parental patience. But for families uncomfortable with crying-based approaches, they’re viable options. The pilot study comparing responsive sleep interventions to extinction methods found both could improve sleep, though with different stress patterns during implementation.
Some families choose to wait out sleep problems entirely, accepting nighttime parenting as temporary. Many infants do eventually consolidate sleep without formal intervention, though the timeline varies dramatically.
The Self-Soothing Myth
Here’s something important: the term “self-soothing” can be misleading. It’s sometimes interpreted as making babies cry it out or ignoring cries. That’s not accurate.
True self-soothing involves babies learning calming strategies—sucking on hands, finding comfortable positions, settling after brief fussiness. This is a developmental skill that emerges gradually. Some babies develop it earlier, others later.
Teaching these skills doesn’t require ignoring all cries. It involves creating opportunities for babies to practice settling while knowing a caregiver is available if genuinely needed. There’s a meaningful difference between allowing a baby to fuss for 3 minutes while finding their thumb versus leaving them to scream for an hour.
The Bottom Line for Exhausted Parents
Is it OK to let a baby cry? The honest answer is: it depends.
Brief, monitored crying during age-appropriate sleep training doesn’t appear to cause attachment damage or developmental harm based on current research. Studies show improvements in both infant sleep and maternal mental health when controlled crying methods are used with older infants who have persistent sleep problems.
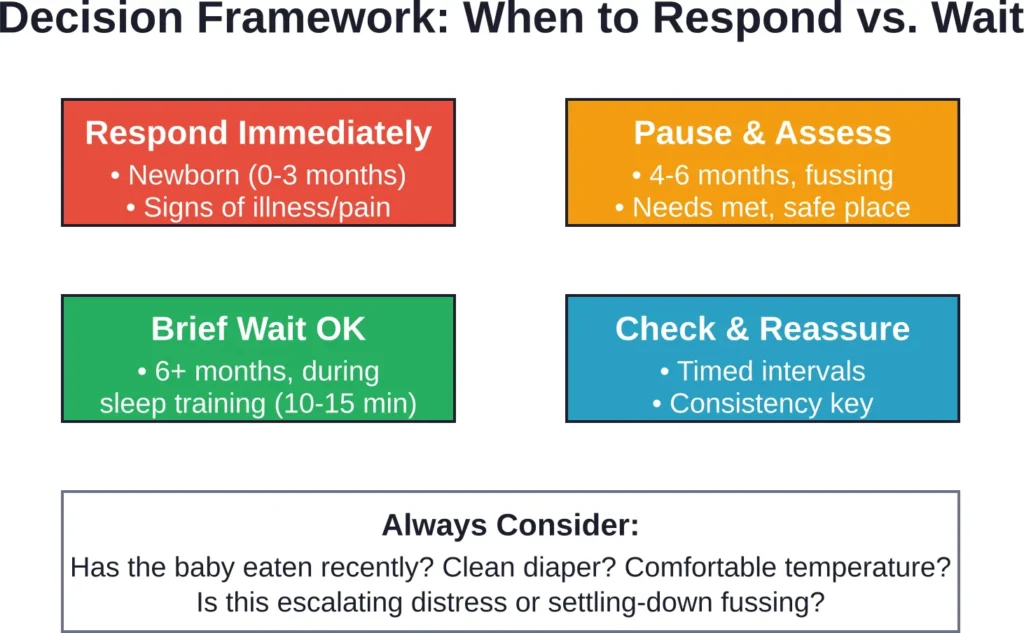
But context is everything. A 6-week-old crying for hunger needs immediate response. A 7-month-old fussing for 5 minutes while learning to settle might not. A baby screaming in escalating distress always needs checking, regardless of age or method.
The research also shows that parental mental health matters enormously. Maternal depression improves when sleep improves. Sleep-deprived parents cannot provide the responsive, sensitive care that supports healthy attachment. Sometimes the most responsive thing parents can do is address their own sleep deprivation.
There’s no single right answer for every family. Some thrive with responsive methods that avoid crying. Others find controlled crying works efficiently for everyone’s wellbeing. Still others muddle through without formal methods.
What matters most? Responding to genuine distress, meeting basic needs consistently, providing overall sensitive and responsive care throughout the day, and preserving parental mental health. Brief crying during sleep learning, when approached thoughtfully, doesn’t override those foundational elements.
Trust yourself to know your baby. If a method feels wrong for your family, it probably is—for your family. But don’t let fear-based messaging convince you that 10 minutes of monitored crying will undo your entire relationship. The research doesn’t support that fear.
Frequently Asked Questions
For young infants under 4 months, prolonged crying should always be investigated and addressed. For older infants during sleep training, 10 to 15 minutes is a reasonable limit before checking. If crying escalates or continues beyond this window despite checks, it’s time to pick up the baby and reassess. Extended crying sessions lasting an hour or more aren’t recommended by mainstream sleep training methods.
Research examining controlled crying methods (with parental checks at intervals) found no association with adverse attachment or behavioral development when practiced in structured ways. The key factor appears to be overall patterns of responsive care throughout the day and across development, not brief crying episodes during sleep teaching. However, these studies examined structured methods with limits, not prolonged unattended distress.
Most pediatric experts recommend waiting until at least 4 to 6 months before attempting formal sleep training methods that involve letting babies cry. Circadian rhythms begin developing around 10 to 12 weeks, but younger infants still have legitimate nighttime feeding needs and are establishing trust and security. The studies showing sleep training benefits involved infants with a mean age of 7 months.
This is extremely common and doesn’t mean something is wrong. Babies are biologically programmed to seek proximity to caregivers. For young infants, responding consistently builds security. For older infants, gradual teaching can help—putting them down drowsy but awake, staying nearby, offering reassurance. If this pattern persists and significantly impacts family functioning by 6 months or later, consulting a pediatrician about age-appropriate sleep strategies makes sense.
The term “cry it out” encompasses a wide range of approaches, from full extinction (rarely recommended by experts) to gentle methods with frequent checks. Research on controlled crying methods shows benefits for infant sleep and maternal mental health without evidence of attachment harm. However, family values differ—what feels appropriate to one family may feel unacceptable to another. Responsive alternatives exist for families uncomfortable with any crying-based approach.
First, systematically check basic needs: hunger, diaper, temperature, signs of illness or pain. Try standard soothing techniques: holding, rocking, singing, white noise, dim lights. If nothing works and you’re becoming frustrated or overwhelmed, place the baby on their back in a safe sleep space and take a brief break. Crying won’t harm the baby, but handling them roughly out of frustration can cause serious injury. Contact your pediatrician if inconsolable crying persists or you notice other concerning symptoms.
Brief cortisol elevations during learning new skills, including sleep, differ from chronic stress exposure. A pilot study examined stress responses during different sleep intervention approaches, finding variation between responsive and extinction methods. However, research also notes that up to 40% of parents report concerning infant sleep disturbance, which creates parental stress that affects infants as well. The relationship between brief crying during sleep training and long-term stress responses remains an active research area with no definitive answers about harm from structured, limited methods.
Making the Decision That Works for Your Family
Evidence provides guidance, but it can’t make individual family decisions. Some families find that controlled crying methods implemented around 6 months solve sleep problems efficiently with minimal distress. Research supports this as a reasonable approach when persistent sleep problems affect family functioning.
Other families choose gentler methods that take longer but involve less crying. Still others decide to wait out sleep challenges without formal intervention, accepting nighttime parenting as a temporary phase.
All of these approaches can work. All have research or experiential support. The best method is the one that aligns with family values, meets the baby’s needs, and preserves parental mental health.
If you’re drowning in sleep deprivation and worried about your mental health, evidence suggests that addressing infant sleep problems can help. If current sleep arrangements work reasonably well for everyone, there’s no requirement to change them.
The key is making an informed choice based on accurate information rather than fear or guilt. Brief, monitored crying during age-appropriate sleep teaching isn’t the catastrophe some sources claim. But it’s also not mandatory. Parents have options.
Whatever approach you choose, remember that overall responsive, sensitive care throughout your baby’s development matters far more than any single parenting decision. Sleep training or not sleep training won’t determine whether your child thrives. Your ongoing relationship will.
Need more specific guidance for your situation? Consult your pediatrician. They can help you determine whether your baby’s sleep patterns are within normal developmental ranges or whether intervention might benefit your family. They can also assess for underlying issues like reflux or other medical conditions that affect sleep and crying.
Above all, be kind to yourself. Parenting a baby is relentlessly demanding. Getting conflicting advice from every direction makes it harder. Trust your knowledge of your baby, use available evidence as a guide, and make the choice that feels right for your family.