
Quick Summary: Gentle straining for brief periods is generally safe after hysterectomy, but excessive pushing should be avoided, especially in the first 4-6 weeks. Straining increases intra-abdominal pressure that can stress healing tissues. Focus on softening stools through hydration, fiber, gentle movement, and stool softeners rather than relying on forceful pushing.
Hysterectomy is one of the most common surgeries in the United States, with hundreds of thousands done each year. While it effectively treats conditions like uterine fibroids, abnormal bleeding, endometriosis, and certain cancers, recovery brings its own set of challenges.
One concern that catches many off guard? Bowel movements. And not just whether they’ll happen, but whether it’s safe to push when they do.
The short answer? It’s complicated. Gentle pushing is usually fine, but hard straining can create problems. Here’s what the research shows and what practical steps actually help during recovery.
Why Bowel Movements Become Difficult After Hysterectomy
Several factors converge to make post-surgical bowel movements more challenging than usual.
Anesthesia slows gut motility — the wave-like muscle contractions that move stool through the intestines. Pain medications, particularly opioids prescribed after surgery, compound this effect significantly. They bind to receptors in the digestive tract, essentially putting the brakes on normal bowel function.
Reduced physical activity during recovery further slows things down. Movement stimulates bowel activity, and when patients spend more time resting (as they should), their digestive system follows suit.
But here’s the thing — surgical changes matter too. Research indicates hysterectomy plays an important role in the pathogenesis of disturbed defecation. The procedure may affect nerve function and anatomical support structures in the pelvic region.
According to research comparing different surgical approaches, bowel dysfunction varies by technique. Research shows bowel dysfunction deterioration rates of 43% after laparoscopic-assisted radical vaginal hysterectomy (LARVH), 47% after vaginal-assisted robotic radical vaginal hysterectomy (VARRVH), and 72% after total minimally invasive radical hysterectomy (TMMR).
Understanding the Risks of Straining
So what actually happens when someone strains hard to pass stool after hysterectomy?
Forceful pushing sharply increases intra-abdominal pressure. That pressure doesn’t stay isolated — it radiates throughout the pelvic cavity, reaching healing surgical sites.
During the first several weeks post-surgery, internal tissues are knitting back together. The vaginal cuff (where the cervix was removed in most cases) is still healing. Excessive pressure can stress these vulnerable areas before they’ve fully mended.
Real talk: the consequences can be serious. Vaginal cuff dehiscence — when the surgical closure separates — occurs in 0.14–4.1% of hysterectomy cases. While not exclusively caused by straining, increased abdominal pressure is a known risk factor. In severe cases, this can lead to evisceration, where internal organs protrude through the opening.
Beyond immediate surgical concerns, chronic straining contributes to pelvic floor dysfunction. The pelvic floor muscles and connective tissue that support pelvic organs can weaken over time with repeated excessive pressure, potentially leading to prolapse issues down the road.
What “Safe” Pushing Actually Means
The distinction between safe and unsafe comes down to degree and duration.
Brief, gentle effort while breathing normally is generally acceptable. Think of it as allowing the natural bearing-down reflex rather than forcing it. This means short periods of mild pressure, not prolonged red-in-the-face straining.
Hold your breath while pushing? That’s a problem. Breath-holding during straining (called the Valsalva maneuver) dramatically increases intra-abdominal pressure beyond what’s created by abdominal muscle contraction alone.
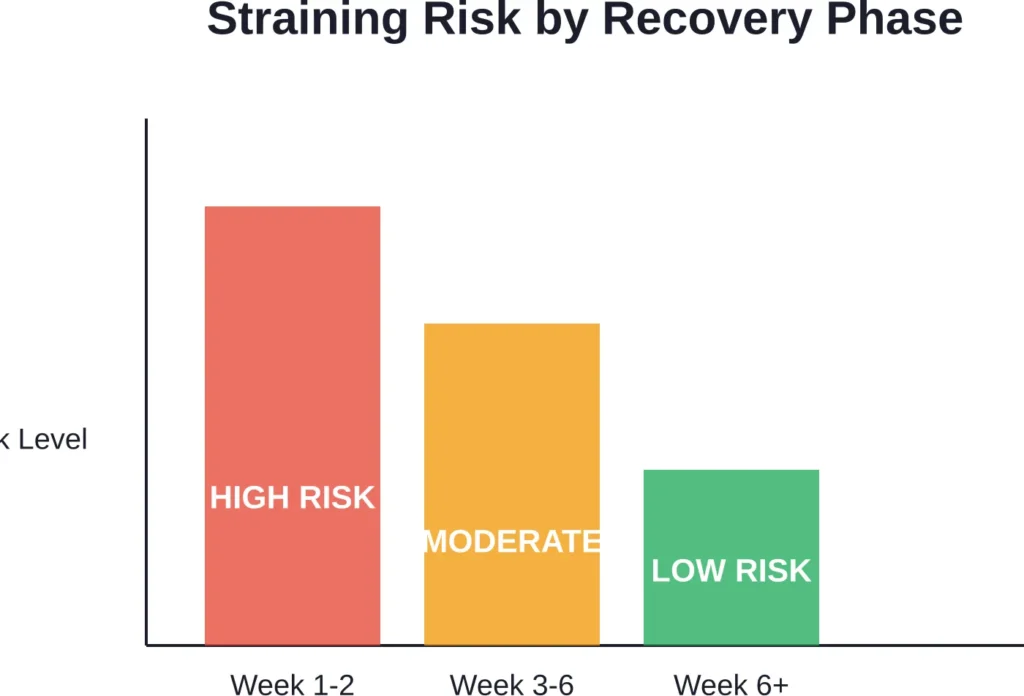
The first four to six weeks represent the highest-risk period. Internal healing progresses significantly during this window, making tissue more vulnerable to disruption. After six weeks, when most patients receive clearance to resume normal activities, tissues have typically healed enough to handle more typical pressures.
That said, the goal throughout recovery should be making bowel movements easy enough that minimal pushing is needed at all.
Research on Post-Hysterectomy Bowel Function
Studies comparing surgical techniques reveal how common bowel changes are after hysterectomy.
Research published in the International Urogynecology Journal examined 207 patients who underwent radical hysterectomy. The study found significant differences in bowel symptoms based on surgical approach:
| Symptom | Abdominal Radical Hysterectomy | Laparoscopic Radical Hysterectomy |
|---|---|---|
| Straining at stool | 19.5% | 1.3% |
| Incomplete defecation | 13.3% | 3.8% |
These numbers tell a story: laparoscopic approaches generally result in fewer bowel complications than open abdominal procedures. But even with minimally invasive techniques, some patients experience changes.
Research comparing minimally invasive approaches found bowel dysfunction with higher deterioration rates in TMMR (72%) versus LARVH (43%) and VARRVH (47%), with correspondingly higher bowel morbidity.
What’s clear across studies? Hysterectomy affects bowel function in a meaningful percentage of patients. Some changes resolve as healing progresses; others persist longer-term.
Proven Strategies to Minimize Straining
The best approach isn’t learning to strain safely — it’s preventing the need to strain in the first place.
Hydration Makes Everything Easier
Water softens stool by keeping it moist as it moves through the colon. Aim for at least eight glasses daily, and more if taking opioid pain medications. Dehydration hardens stool quickly, making it harder to pass.
Fiber Timing Matters
Dietary fiber helps, but timing is critical. During the first days after surgery, a lighter diet is typically recommended. As recovery progresses and appetite returns, gradually increase fiber intake through fruits, vegetables, whole grains, and legumes.
Research on dietary management after radical hysterectomy suggests that dietary fiber represents an inexpensive, effective therapeutic intervention for addressing bowel dysfunction. But ramp up slowly — too much fiber too fast can cause gas and bloating when the gut is still sluggish.
Stool Softeners vs. Laxatives
Stool softeners like docusate work by drawing water into the stool, making it easier to pass. They’re generally safe for post-surgical use and don’t stimulate contractions.
Stimulant laxatives trigger intestinal contractions. While sometimes necessary, they’re not the first choice immediately after surgery. Check with healthcare providers before using any laxative products.
Movement Stimulates the Gut
Even gentle walking encourages bowel activity. Start with short walks as soon as cleared by the surgical team — often within hours of abdominal hysterectomy or the same day for vaginal or laparoscopic approaches.
Movement increases blood flow, stimulates peristalsis, and helps gas move through the system. It doesn’t need to be vigorous; consistent, gentle activity works.
Positioning on the Toilet
Body position affects how easy it is to pass stool. Elevating feet on a small stool while sitting on the toilet straightens the anorectal angle, making evacuation easier with less straining.
This position mimics squatting, which is biomechanically optimal for defecation. A 6-9 inch footstool typically works well for standard toilet heights.
Timeline: What to Expect Week by Week
Recovery isn’t linear, but there are general patterns most patients follow.
Week 1-2: The Constipation Zone
This is typically when bowel movements are most difficult. Anesthesia effects linger, pain medications peak, and activity is minimal. Many patients don’t have a bowel movement for 3-5 days post-surgery.
Some women experience an increase in vaginal bleeding around two weeks post-surgery, which is normal. This typically lasts 24 hours. If it becomes very heavy or persists, contact the healthcare provider.
Week 3-6: Gradual Improvement
As pain decreases and medication tapers, bowel function typically improves. Activity increases, appetite normalizes, and the gut starts moving more regularly.
This is still the healing window where caution matters. Tissues are stronger than week one but not fully healed. Gentle pushing is generally safe, but hard straining should still be avoided.
Beyond 6 Weeks: The New Normal
Most patients receive clearance to resume all normal activities around six weeks. By this point, bowel function has often returned to baseline or close to it.
However, some women experience longer-term changes. Community discussions note that some individuals deal with ongoing bowel sensitivity or altered function months after surgery. These cases warrant follow-up with healthcare providers.
Warning Signs That Require Medical Attention
While some bowel changes are expected, certain symptoms need prompt evaluation.
Seek medical help if experiencing:
- Fever of 100.4° F (38° C) or higher
- Redness, swelling, tenderness, drainage from your wound or opening in operative site
- No bowel movement for more than 5-7 days despite stool softeners and dietary measures
- Severe abdominal pain
- Nausea and vomiting that prevent keeping fluids down
- Bright red blood in stool or black, tarry stools
- Feeling or seeing tissue protruding from the vagina
These symptoms could indicate complications like infection, cuff dehiscence, or intestinal obstruction. Early intervention prevents more serious problems.
Long-Term Bowel Health After Hysterectomy
Once initial healing completes, maintaining bowel health becomes about sustainable habits.
Research indicates hysterectomy can play a role in long-term disturbed defecation for some patients. While many women return to completely normal function, others notice persistent changes.
Maintaining adequate fiber intake (25-30 grams daily for most women), staying hydrated, and keeping physically active form the foundation of good bowel health. These habits prevent the chronic constipation that leads to habitual straining.
Pelvic floor physical therapy can help for those experiencing ongoing issues. Specialized therapists teach proper bowel habits, pelvic floor coordination, and techniques to improve function without straining.
Managing Pain Medication and Bowel Function
Opioid pain medications create a tough trade-off: they control post-surgical pain effectively but essentially guarantee constipation.
These medications activate opioid receptors throughout the digestive tract, slowing motility and increasing fluid absorption from stool. The result is harder, drier stool that’s difficult to pass.
Strategies to manage this include:
Starting stool softeners immediately when beginning opioids, not waiting for constipation to develop. Prevention is far easier than treating established constipation.
Tapering off opioids as soon as pain allows. Many patients can switch to non-opioid pain relievers like acetaminophen or ibuprofen within a few days, especially after minimally invasive procedures.
Discussing medication alternatives with the surgical team. Some patients do well with non-opioid pain management from the start, though this depends on individual pain levels and the surgical approach used.
When Different Surgical Approaches Matter
The type of hysterectomy performed influences bowel complications.
Abdominal hysterectomy involves a larger incision and more tissue disruption. Studies show higher rates of bowel symptoms like straining (19.5%) and incomplete defecation (13.3%) compared to laparoscopic approaches.
Laparoscopic and robotic procedures use smaller incisions and typically involve less tissue trauma. Research shows significantly lower rates of straining (1.3%) and incomplete defecation (3.8%) with laparoscopic radical hysterectomy.
Vaginal hysterectomy, when feasible, often results in the quickest return to normal bowel function since there’s no abdominal incision at all.
Radical hysterectomy (removing more tissue for cancer treatment) carries higher risks than simple hysterectomy. The more extensive dissection affects nerves and blood supply in the pelvis, potentially impacting long-term bowel function.
| Procedure Type | Straining Rate | Incomplete Defecation Rate |
|---|---|---|
| Abdominal Radical | 19.5% | 13.3% |
| Laparoscopic Radical | 1.3% | 3.8% |
| Simple (any approach) | Lower than radical | Lower than radical |
Frequently Asked Questions
Most surgeons recommend avoiding forceful straining for at least 4-6 weeks while internal tissues heal. After clearance at the six-week follow-up, normal bowel habits can typically resume. Gentle pushing is usually acceptable earlier, but hard, prolonged straining should be avoided during the initial healing period. The goal throughout recovery is softening stools enough that minimal pushing is needed.
Contact the surgical team or primary care provider. Going five days without a bowel movement isn’t uncommon after surgery, but it warrants intervention. Healthcare providers may recommend specific laxatives, suppositories, or enemas. Don’t wait beyond 5-7 days to seek guidance, as prolonged constipation becomes harder to resolve and increases the temptation to strain excessively.
Yes, excessive straining can potentially contribute to vaginal cuff dehiscence, where the internal surgical closure separates. This occurs in 0.14–4.1% of hysterectomy cases. While multiple factors contribute to this complication, increased abdominal pressure from straining is a known risk factor, particularly in the first six weeks. This is why preventing constipation and avoiding forceful pushing is emphasized during recovery.
Stool softeners like docusate are generally safe for daily use during the recovery period and beyond if needed. They work by drawing water into stool rather than stimulating the intestines. Many surgeons recommend starting them immediately after surgery and continuing until bowel function normalizes. Long-term daily use is typically safe, though addressing underlying causes of constipation through diet and lifestyle is preferable for ongoing management.
Most women return to normal or near-normal bowel function within weeks to months after hysterectomy. However, research indicates some patients experience longer-term changes. Simple hysterectomy typically has better outcomes than radical procedures. Factors affecting recovery include surgical approach, extent of dissection, individual healing, and pre-existing bowel conditions. If bowel symptoms persist beyond three months, consultation with a gastroenterologist or pelvic floor specialist may help.
Rather than focusing on foods to avoid, emphasize foods that help: fruits, vegetables, whole grains, and adequate fluids. However, in the first few days when appetite is low and the gut is sluggish, very heavy or gas-producing foods might be uncomfortable. Start with lighter, easily digestible options and progress as tolerated. Avoid excessive cheese and processed foods, which can be constipating. The key is gradually increasing fiber as recovery progresses.
Some discomfort is common, especially in the first week or two. Abdominal incisions and internal healing can make the muscles used during bowel movements tender. However, sharp pain, severe pain, or pain that worsens over time isn’t normal and should be evaluated. Pain during bowel movements can indicate constipation, hemorrhoids, or less commonly, complications. Using stool softeners, proper positioning, and gentle technique helps minimize discomfort.
The Bottom Line on Post-Hysterectomy Bowel Movements
So is it OK to push to poop after hysterectomy? Gentle, brief pushing while breathing normally is generally safe once bowel function returns. But the real goal is preventing situations where hard straining becomes necessary.
Start prevention strategies immediately: hydration, stool softeners, gentle movement, and dietary adjustments as recovery allows. These measures work far better than trying to strain safely.
Listen to the body. If passing stool requires prolonged, forceful effort that leaves someone exhausted or in pain, that’s a signal to seek help rather than push harder.
Most women navigate post-hysterectomy bowel changes successfully with proper preparation and patience. The first few weeks require extra attention, but bowel function typically improves steadily as healing progresses. When concerns arise, early communication with healthcare providers prevents complications and provides peace of mind.
Recovery from hysterectomy is a process, and bowel function is just one piece. But it’s an important piece — one that significantly affects comfort and quality of life during healing. With the right strategies, this aspect of recovery can be managed effectively, allowing focus on the overall return to health and activity.