
Quick Summary: Elevating your legs for extended periods can lead to complications including deep vein thrombosis (DVT), muscle atrophy, joint stiffness, and cardiovascular issues. While short-term leg elevation (15-30 minutes several times daily) offers health benefits, prolonged immobilization disrupts blood flow, weakens muscles, and can trigger blood clot formation. The key is balancing elevation with regular movement and proper positioning.
Leg elevation is widely recommended for reducing swelling, easing varicose vein symptoms, and improving circulation. Healthcare professionals routinely advise patients to elevate their legs above heart level to combat various conditions.
But here’s the thing—more isn’t always better.
When leg elevation extends beyond therapeutic durations, the body responds in ways that can undermine the very benefits you’re seeking. The line between helpful and harmful is surprisingly thin.
The Double-Edged Nature of Prolonged Elevation
Leg elevation works by using gravity to assist venous return—the process of blood flowing back to the heart. For short periods, this reduces pressure on leg veins and helps drain excess fluid from tissues.
Research published in BMJ (1998) emphasizes that elevation and compression are important—and too often forgotten. However, the same research notes that young adults have required above-the-knee amputations due to complications from improper elevation protocols.
The recommended duration is clear: elevate legs for about 15 minutes, three to four times daily. Going beyond this without movement introduces risk.
What Counts as “Too Long”?
Extended immobilization typically means remaining in one position for hours without interruption. This includes:
- Sleeping with legs elevated for entire nights (6-8 hours continuously)
- Remaining in bed with legs raised for multiple hours during the day
- Post-surgical positioning that extends beyond medical guidance
- Continuous prone or supine positioning exceeding recommended timeframes
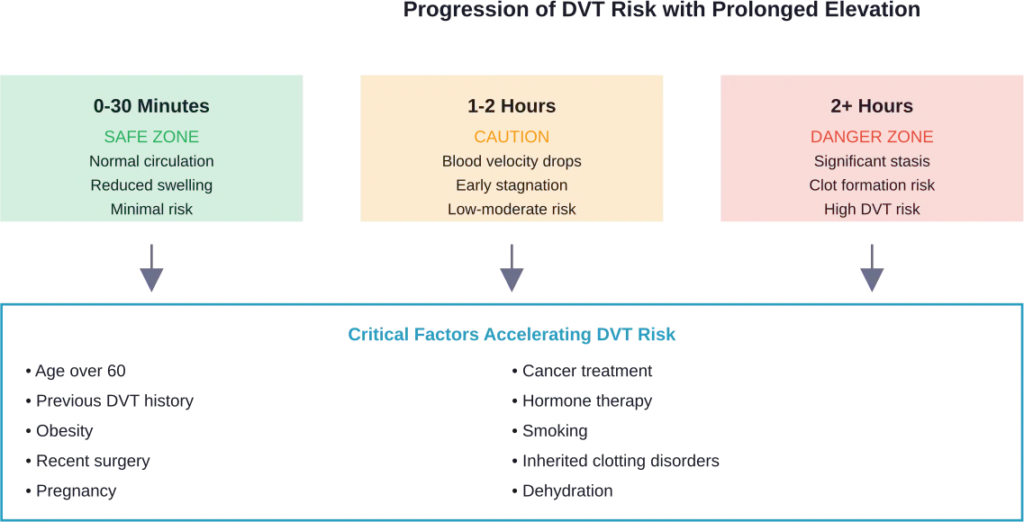
Even two hours of uninterrupted leg elevation can trigger physiological changes that compromise circulation and muscle function.
Deep Vein Thrombosis: The Primary Danger
Prolonged immobilization is a well-established risk factor for DVT—blood clots that form in deep veins, typically in the legs. According to the American Heart Association, hypercoagulability (excessive blood clotting tendency) becomes dangerous when clots form in or travel to arteries or veins of vital organs.
Here’s where it gets concerning. The National Institutes of Health documents cases where continuous prone positioning after retinal detachment surgery led to DVT. A 56-year-old woman without previous underlying disease developed deep vein thrombosis directly attributable to prolonged immobilization.
Traditional medical thinking assumed bed rest prevented pulmonary embolism in DVT patients. Research now shows this approach was fundamentally flawed. Fear of pulmonary embolism kept patients immobilized, but the immobilization itself contributed to clot formation.
How Blood Clots Form During Prolonged Elevation
When legs remain elevated and immobile for hours, blood velocity in leg veins decreases dramatically. This stagnation, combined with the body’s natural clotting mechanisms, creates ideal conditions for thrombus formation.
The BMJ editorial notes that once swelling resolves—usually after only 48 hours of elevation—patients should be mobilized in class II elastic stockings rather than continuing bed rest.
Muscle Atrophy and Skeletal Deterioration
Research on extended bed rest reveals alarming speed at which muscles deteriorate. Academic studies show that prolonged immobility triggers rapid reductions in muscle mass and bone mineral density, with measurable changes appearing within the first week of bed rest.
The critical care environment provides extensive documentation of this phenomenon. When patients remain immobilized—even in therapeutic positions like leg elevation—muscle protein synthesis decreases while protein breakdown accelerates.
Muscle doesn’t just shrink. It fundamentally changes at the cellular level.
The Metabolic Shift
A study from UC Irvine (published February 24, 2026) revealed metabolic triggers that guide muscle repair and growth. When muscles remain inactive for extended periods during leg elevation, these metabolic pathways reverse. Instead of building and repairing tissue, the body begins catabolizing muscle for energy.
Interestingly, research on hibernating squirrels shows that some animals activate endurance exercise pathways despite prolonged immobilization. Humans lack this protective mechanism, making us particularly vulnerable to muscle loss during extended elevation.
Cardiovascular Complications Beyond DVT
The cardiovascular system responds to leg positioning in complex ways. Research presented to the American Heart Association indicates that high blood pressure while lying down (supine hypertension) represents an independent risk factor for heart disease, stroke, heart failure, and premature death.
Participants in the study had blood pressure measured while lying flat. Those with elevated readings in this position faced higher cardiovascular risks compared to adults without supine hypertension, even when seated blood pressure was normal.
This matters for anyone elevating legs for hours. The supine or semi-reclined position alters hemodynamics—the forces governing blood flow through the cardiovascular system.
Prolonged Sitting Leg Vasculopathy
Research published in the American Journal of Physiology examined how prolonged sitting affects leg vasculature. Scientists measured popliteal artery blood flow with subjects lying on their side straight (0° angles) versus lying on their side with hips and knees bent at 90 degrees (mimicking sitting position).
The bent position significantly reduced blood flow. This finding extends to elevated positions where knees remain bent for hours, creating similar vascular compression and flow restriction.
Joint Stiffness and Reduced Mobility
Extended periods in any fixed position cause joints to stiffen. Synovial fluid—the lubricant inside joints—relies on movement to maintain proper viscosity and distribution.
When legs remain elevated and motionless, several things happen:
- Knee joints develop flexion contractures (permanent bending)
- Ankle joints lose dorsiflexion range of motion
- Hip flexors tighten and shorten
- Connective tissue loses elasticity
Research reviewed by the National Institute for Occupational Safety and Health has documented that prolonged static positions—whether standing or lying—contribute to musculoskeletal disorders. Duration of immobility correlates directly with symptom severity.
Proper Leg Elevation Techniques
Safe leg elevation requires attention to positioning, duration, and frequency. Evidence-based practice recommends:
| Factor | Recommendation | Rationale |
|---|---|---|
| Duration | 15-30 minutes per session | Allows fluid drainage without compromising circulation |
| Frequency | 3-4 times daily | Maintains benefits while permitting normal activity |
| Height | Above heart level | Uses gravity to assist venous return |
| Knee position | Slight bend, not locked straight | Prevents joint strain and vascular compression |
| Support | Pillow or wedge under calves | Distributes pressure, avoids hanging feet |
If legs can’t reach heart level, resting them on a coffee table or ottoman still provides some benefit by slowing gravity’s effects.
Common Mistakes That Increase Risk
Vascular specialists identify several errors that transform beneficial elevation into harmful immobilization:
Elevating overnight: Eight hours of continuous elevation during sleep dramatically increases DVT risk. The body needs positional variety and movement during rest.
Allowing feet to hang: When only the thighs are elevated, feet dangling off the edge of furniture creates pressure points and restricts circulation to the lower leg and foot.
Locking knees straight: Hyperextended knees compress popliteal vessels behind the knee, reducing blood flow.
Skipping compression: As BMJ research notes, compression stockings are crucial companions to elevation. Elastic support prevents venous pooling even during brief elevation periods.

Special Populations at Higher Risk
Certain groups face amplified dangers from prolonged leg elevation. Medical research identifies specific vulnerabilities:
Post-surgical patients: Already at elevated DVT risk, these individuals require carefully balanced elevation protocols. Medical supervision ensures elevation supports healing without triggering clot formation.
Pregnant women: Pregnancy increases blood clotting factors naturally. Extended leg elevation without movement compounds this risk. Short elevation sessions help with pregnancy-related swelling, but overnight elevation should be avoided.
Elderly individuals: Age-related decreases in circulation and muscle mass make older adults particularly susceptible to both DVT and rapid muscle atrophy during prolonged elevation.
High-altitude residents: Research on venous thromboembolism after total shoulder arthroplasty found that higher altitude represents an independent risk factor for VTE. Physiological changes at altitude predispose individuals to DVT, making prolonged immobilization even more dangerous.
When to Seek Medical Attention
Mayo Clinic guidelines specify warning signs requiring immediate medical evaluation. Call emergency services if leg swelling occurs with:
- Chest pain or difficulty breathing (possible pulmonary embolism)
- Severe, sudden leg pain with color changes
- Warmth and tenderness in one leg but not the other
- Leg swelling after prolonged immobilization
- Fever accompanying leg symptoms
These symptoms suggest DVT or pulmonary embolism—life-threatening conditions requiring urgent treatment.
Balancing Elevation Benefits with Movement
The solution isn’t abandoning leg elevation. The therapeutic benefits for edema, varicose veins, and wound healing remain well-documented. Rather, the approach requires strategic timing and integration with activity.
According to the American Heart Association, regular exercise lowers blood clot risk. As a general goal, aim for at least 30 minutes of moderate physical activity daily. Combine this with strategic elevation sessions, and you maximize benefits while minimizing risks.
An example of an optimal schedule might include:
- Morning: 20-minute elevation after waking
- Midday: Brief elevation after lunch while wearing compression stockings
- Afternoon: 15-minute elevation session
- Evening: Final 20-minute session before bed
- Between sessions: Normal activity, walking, gentle movement
This pattern provides cumulative elevation benefits without the continuous immobilization that triggers complications.
Alternative Circulation Support Methods
Several complementary strategies enhance circulation without requiring prolonged elevation:
| Method | How It Works | Best For |
|---|---|---|
| Compression stockings | Apply graduated pressure to prevent venous pooling | Varicose veins, chronic venous insufficiency |
| Ankle pumps | Contract calf muscles to pump blood upward | Preventing DVT during sitting or bed rest |
| Walking | Engages muscle pump mechanism naturally | General circulation, preventing stagnation |
| Hydration | Maintains blood viscosity and flow properties | All circulation concerns |
| Position changes | Prevents prolonged pressure on any vessel | Bed-bound or mobility-limited individuals |
These methods work synergistically with appropriate elevation to support vein health and circulation.
Frequently Asked Questions
The safest duration is 15-30 minutes per session, repeated three to four times daily. This provides therapeutic benefits without triggering circulation problems or increasing DVT risk. Avoid continuous elevation exceeding two hours without movement breaks.
Yes, sleeping with legs elevated for entire nights (6-8 hours) increases DVT risk due to prolonged immobilization. The extended period without movement allows blood to pool and stagnate in leg veins, creating conditions favorable for clot formation. Short elevation before sleep is fine, but don’t maintain the position all night.
Warning signs include severe leg pain, warmth and redness in one leg, sudden swelling after prolonged elevation, numbness or tingling that doesn’t resolve quickly, and difficulty moving the leg normally after elevation. Any chest pain or breathing difficulty after leg elevation requires immediate emergency care.
Multiple short sessions spread throughout the day are significantly safer and often more effective than single prolonged sessions. Three to four 15-20 minute elevation periods provide cumulative benefits while allowing normal activity and circulation between sessions.
While legs should be above heart level for optimal fluid drainage, extremely high elevation (legs vertical against a wall for extended periods) can cause discomfort and isn’t necessary. A 15-30 degree angle above heart level provides adequate gravitational assistance without strain.
Yes, medical research strongly supports combining compression stockings with leg elevation. The compression prevents venous pooling and supports the beneficial effects of elevation while reducing DVT risk. This combination is more effective than elevation alone.
Previous DVT history, recent surgery, pregnancy, cancer treatment, obesity, age over 60, smoking, inherited clotting disorders, and high-altitude residence all increase risks associated with prolonged elevation. People with these factors should consult healthcare providers before beginning elevation routines and strictly limit duration.
Conclusion: Finding the Right Balance
Leg elevation remains a valuable therapeutic tool when used appropriately. The evidence clearly shows benefits for managing swelling, supporting vein health, and accelerating wound healing.
But those benefits evaporate—and transform into serious health risks—when elevation becomes prolonged immobilization. DVT, muscle atrophy, joint stiffness, and cardiovascular complications represent real dangers that emerge surprisingly quickly.
The key lies in strategic, time-limited elevation sessions combined with compression support and regular movement. Fifteen to thirty minutes, three to four times daily, provides therapeutic benefits without crossing into dangerous territory.
If you’re currently using leg elevation for symptom management, review your approach against evidence-based guidelines. Consult a healthcare provider about optimal duration and frequency for your specific situation. Don’t assume that more elevation automatically means better results—sometimes less is genuinely more when it comes to protecting your vascular and musculoskeletal health.